Serotype-Specific Changes in Invasive Pneumococcal Disease after Pneumococcal Conjugate Vaccine Introduction: A Pooled Analysis of Multiple Surveillance Sites
Supporting Files
Public Domain

-
Sep 24 2013
-
File Language:
English
Details
-
Alternative Title:PLoS Med
-
Personal Author:
-
Corporate Authors:
-
Description:In a pooled analysis of data collected from invasive pneumococcal disease surveillance databases, Daniel Feikin and colleagues examine serotype replacement after the introduction of 7-valent pneumococcal conjugate vaccine (PCV7) into national immunization programs.
Background
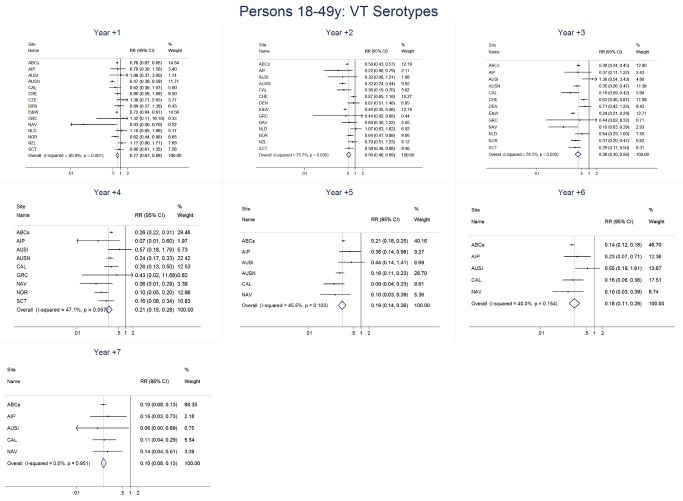
Vaccine-serotype (VT) invasive pneumococcal disease (IPD) rates declined substantially following introduction of 7-valent pneumococcal conjugate vaccine (PCV7) into national immunization programs. Increases in non-vaccine-serotype (NVT) IPD rates occurred in some sites, presumably representing serotype replacement. We used a standardized approach to describe serotype-specific IPD changes among multiple sites after PCV7 introduction.
Methods and Findings
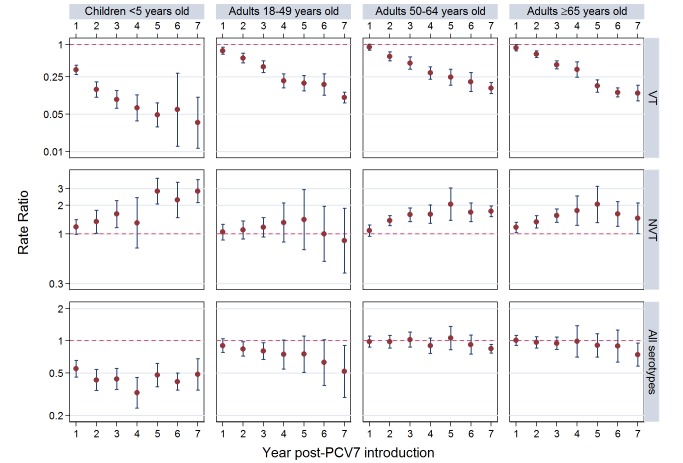
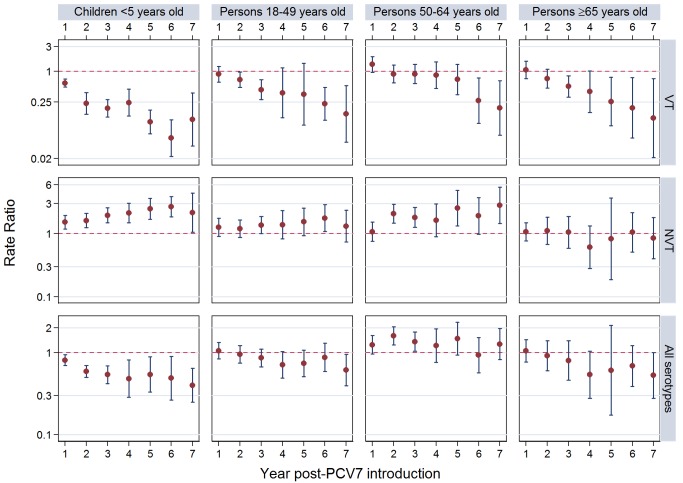
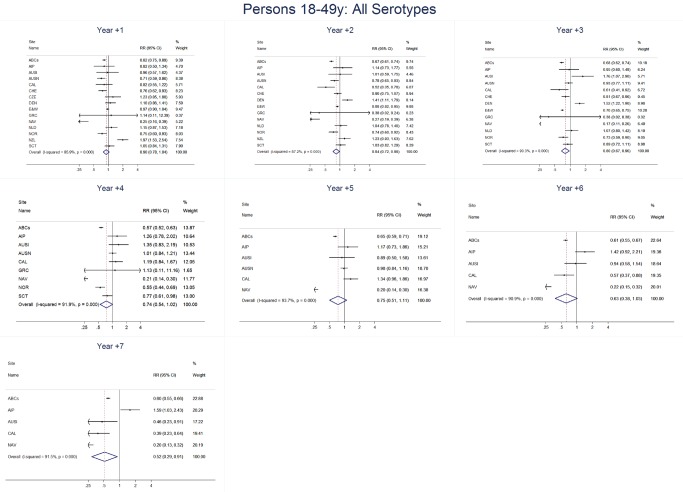
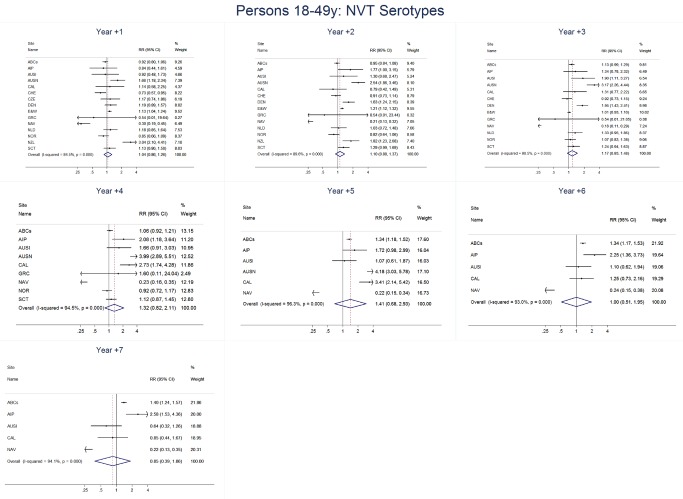
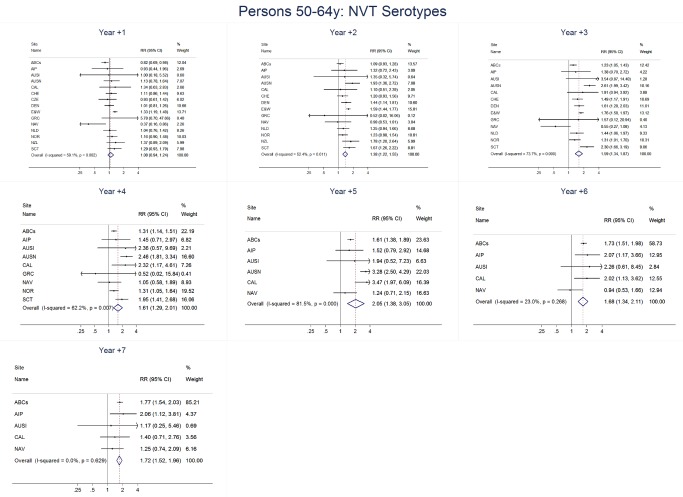
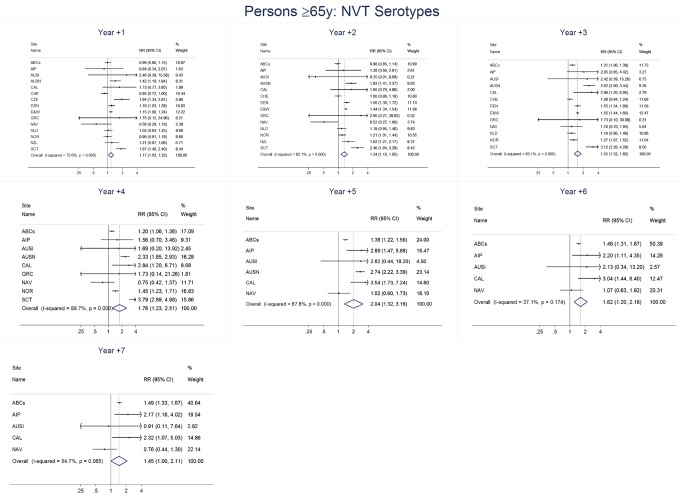
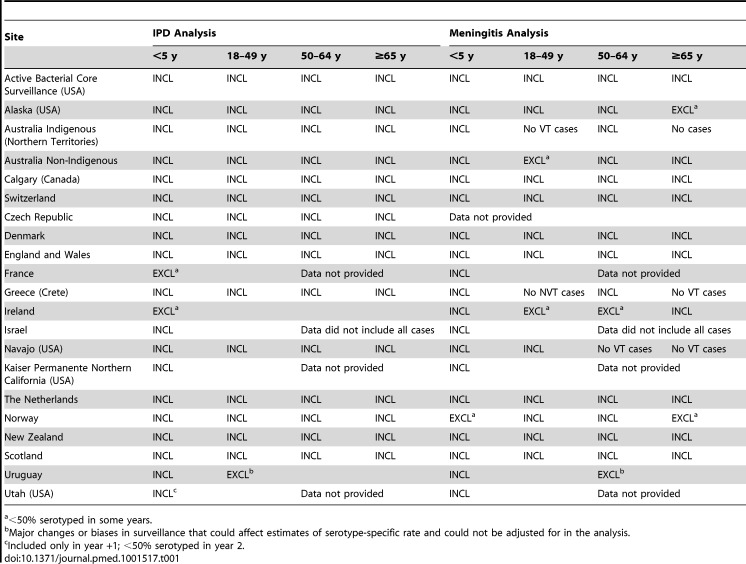
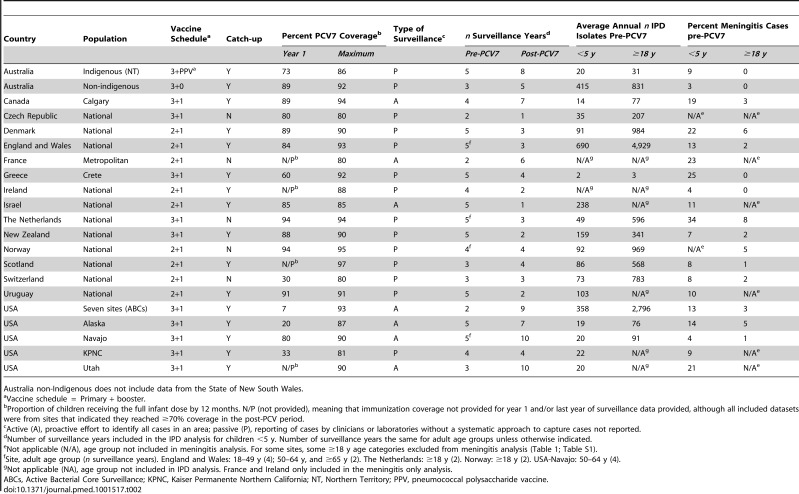
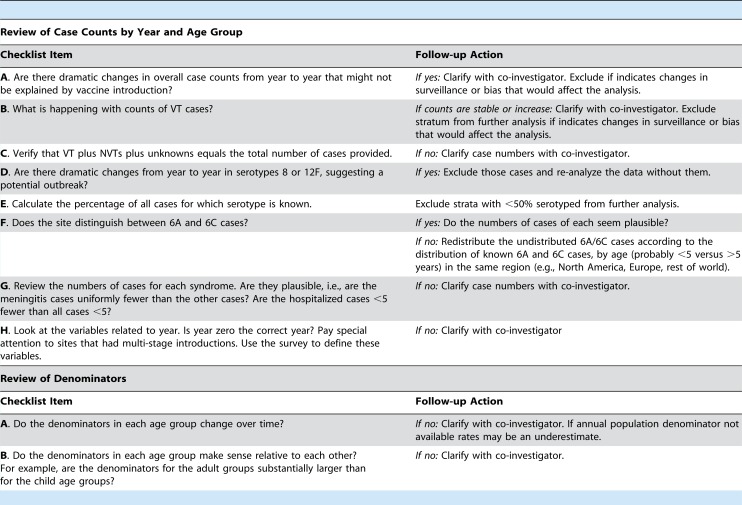
Of 32 IPD surveillance datasets received, we identified 21 eligible databases with rate data ≥2 years before and ≥1 year after PCV7 introduction. Expected annual rates of IPD absent PCV7 introduction were estimated by extrapolation using either Poisson regression modeling of pre-PCV7 rates or averaging pre-PCV7 rates. To estimate whether changes in rates had occurred following PCV7 introduction, we calculated site specific rate ratios by dividing observed by expected IPD rates for each post-PCV7 year. We calculated summary rate ratios (RRs) using random effects meta-analysis. For children <5 years old, overall IPD decreased by year 1 post-PCV7 (RR 0·55, 95% CI 0·46–0·65) and remained relatively stable through year 7 (RR 0·49, 95% CI 0·35–0·68). Point estimates for VT IPD decreased annually through year 7 (RR 0·03, 95% CI 0·01–0·10), while NVT IPD increased (year 7 RR 2·81, 95% CI 2·12–3·71). Among adults, decreases in overall IPD also occurred but were smaller and more variable by site than among children. At year 7 after introduction, significant reductions were observed (18–49 year-olds [RR 0·52, 95% CI 0·29–0·91], 50–64 year-olds [RR 0·84, 95% CI 0·77–0·93], and ≥65 year-olds [RR 0·74, 95% CI 0·58–0·95]).
Conclusions
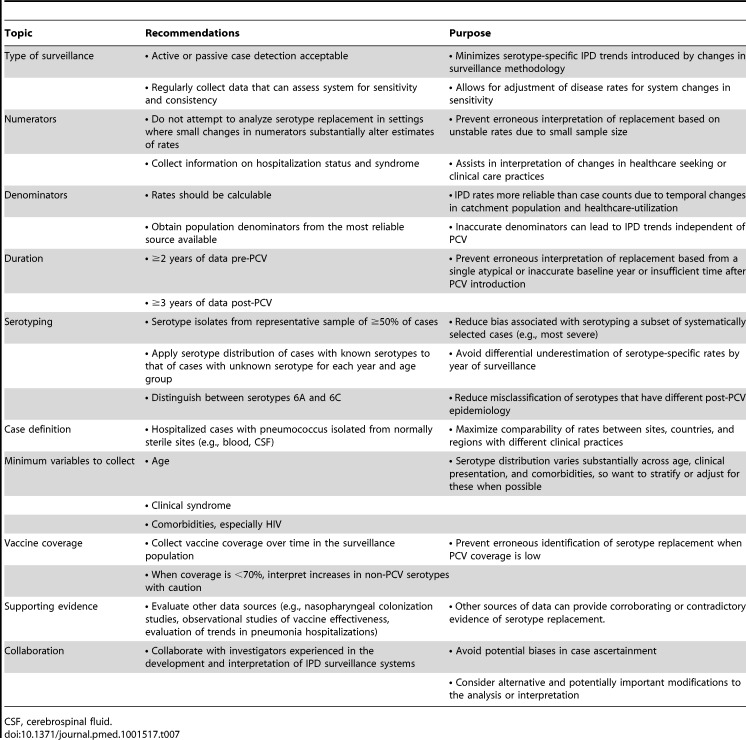
Consistent and significant decreases in both overall and VT IPD in children occurred quickly and were sustained for 7 years after PCV7 introduction, supporting use of PCVs. Increases in NVT IPD occurred in most sites, with variable magnitude. These findings may not represent the experience in low-income countries or the effects after introduction of higher valency PCVs. High-quality, population-based surveillance of serotype-specific IPD rates is needed to monitor vaccine impact as more countries, including low-income countries, introduce PCVs and as higher valency PCVs are used.
Pneumococcal disease–a major cause of illness and death in children and adults worldwide–is caused by Streptococcus pneumoniae, a bacterium that often colonizes the nose and throat harmlessly. Unfortunately, S. pneumoniae occasionally spreads into the lungs, bloodstream, or covering of the brain, where it causes pneumonia, septicemia, and meningitis, respectively. These invasive pneumococcal diseases (IPDs) can usually be successfully treated with antibiotics but can be fatal. Consequently, it is better to avoid infection through vaccination. Vaccination primes the immune system to recognize and attack disease-causing organisms (pathogens) rapidly and effectively by exposing it to weakened or dead pathogens or to pathogen molecules that it recognizes as foreign (antigens). Because there are more than 90 S. pneumoniae variants or “serotypes,” each characterized by a different antigenic polysaccharide (complex sugar) coat, vaccines that protect against S. pneumoniae have to include multiple serotypes. Thus, the pneumococcal conjugate vaccine PCV7, which was introduced into the US infant immunization regimen in 2000, contains polysaccharides from the seven S. pneumoniae serotypes mainly responsible for IPD in the US at that time.
Why Was This Study Done?
Vaccination with PCV7 was subsequently introduced in several other high- and middle-income countries, and IPD caused by the serotypes included in the vaccine declined substantially in children and in adults (because of reduced bacterial transmission and herd protection) in the US and virtually all these countries. However, increases in IPD caused by non-vaccine serotypes occurred in some settings, presumably because of “serotype replacement.” PCV7 prevents both IPD caused by the serotypes it contains and carriage of these serotypes. Consequently, after vaccination, previously less common, non-vaccine serotypes can colonize the nose and throat, some of which can cause IPD. In July 2010, a World Health Organization expert consultation on serotype replacement called for a comprehensive analysis of the magnitude and variability of pneumococcal serotype replacement following PCV7 use to help guide the introduction of PCVs in low-income countries, where most pneumococcal deaths occur. In this pooled analysis of data from multiple surveillance sites, the researchers investigate serotype-specific changes in IPD after PCV7 introduction using a standardized approach.
What Did the Researchers Do and Find?
The researchers identified 21 databases that had data about the rate of IPD for at least 2 years before and 1 year after PCV7 introduction. They estimated whether changes in IPD rates had occurred after PCV7 introduction by calculating site-specific rate ratios–the observed IPD rate for each post-PCV7 year divided by the expected IPD rate in the absence of PCV7 extrapolated from the pre-PCV7 rate. Finally, they used a statistical approach (random effects meta-analysis) to estimate summary (pooled) rate ratios. For children under 5 years old, the overall number of observed cases of IPD in the first year after the introduction of PCV7 was about half the expected number; this reduction in IPD continued through year 7 after PCV7 introduction. Notably, the rate of IPD caused by the S. pneumonia serotypes in PCV7 decreased every year, but the rate of IPD caused by non-vaccine serotypes increased annually. By year 7, the number of cases of IPD caused by non-vaccine serotypes was 3-fold higher than expected, but was still smaller than the decrease in vaccine serotypes, thereby leading to the decrease in overall IPD. Finally, smaller decreases in overall IPD also occurred among adults but occurred later than in children 2 years or more after PCV7 introduction.
What Do These Findings Mean?
These findings show that consistent, rapid, and sustained decreases in overall IPD and in IPD caused by serotypes included in PCV7 occurred in children and thus support the use of PCVs. The small increases in IPD caused by non-vaccine serotypes that these findings reveal are likely to be the result of serotype replacement, but changes in antibiotic use and other factors may also be involved. These findings have several important limitations, however. For example, PCV7 is no longer made and extrapolation of these results to newer PCV10 and PCV13 formulations should be done cautiously. On the other hand, many of the serotypes causing serotype replacement after PCV7 are included in these higher valency vaccines. Moreover, because the data analyzed in this study mainly came from high-income countries, these findings may not be generalizable to low-income countries. Nevertheless, based on their analysis, the researchers make recommendations for the collection and analysis of IPD surveillance data that should allow valid interpretations of the effect of PCVs on IPD to be made, an important requisite for making sound policy decisions about vaccination against pneumococcal disease.
Additional Information
Please access these websites via the online version of this summary at http://dx.doi.org/10.1371/journal.pmed.1001517.
-
Subjects:
-
Source:PLoS Med. 2013; 10(9).
-
Document Type:
-
Volume:10
-
Issue:9
-
Collection(s):
-
Main Document Checksum:urn:sha256:23540be14ccc38ba1ed7cf00b02e7d0504e4b56ae0aa1fd96bee9d841be76d65
-
Download URL:
-
File Type:
 [PDF
- 3.24 MB
]
[PDF
- 3.24 MB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access