Rising Bilateral Mastectomy Rates Among Neoadjuvant Chemotherapy Recipients in California, 1998–2012
Supporting Files

-
Aug 2017
-
File Language:
English
Details
-
Alternative Title:Ann Surg
-
Personal Author:
-
Description:Background
Neoadjuvant chemotherapy (NAC) for operable breast cancer (BC) can downstage disease and facilitate breast conservation.
Objective
To assess trends in NAC use and surgical procedures in California from 1/1/1998 to 12/31/2012 using statewide population-based cancer registry data.
Methods
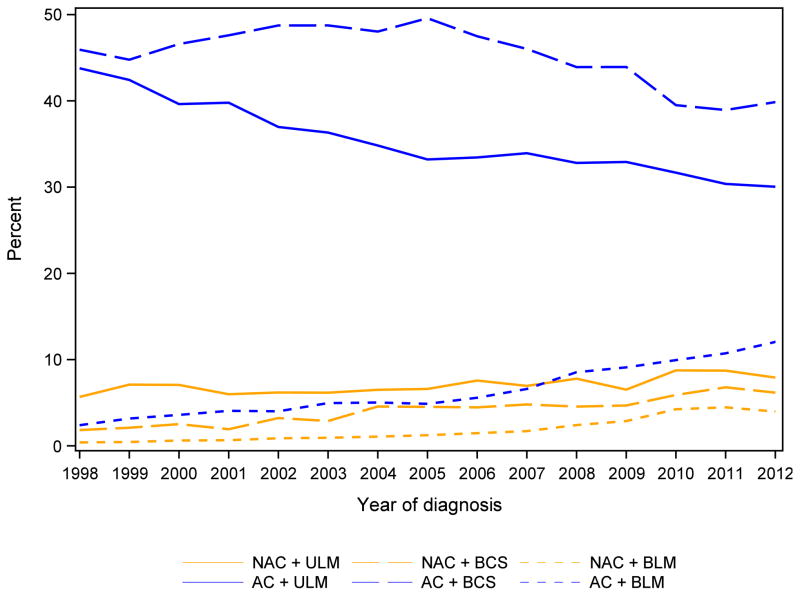
236,797 women diagnosed with stage I–III BC were studied. Information regarding NAC, adjuvant chemotherapy (aCT), breast conserving surgery (BCS), bilateral mastectomy (BLM) and unilateral mastectomy (ULM) was abstracted from the medical records. Multivariable polytomous logistic regression were used to estimate odds ratios (OR) of receiving NAC and of type of surgery after NAC.
Results
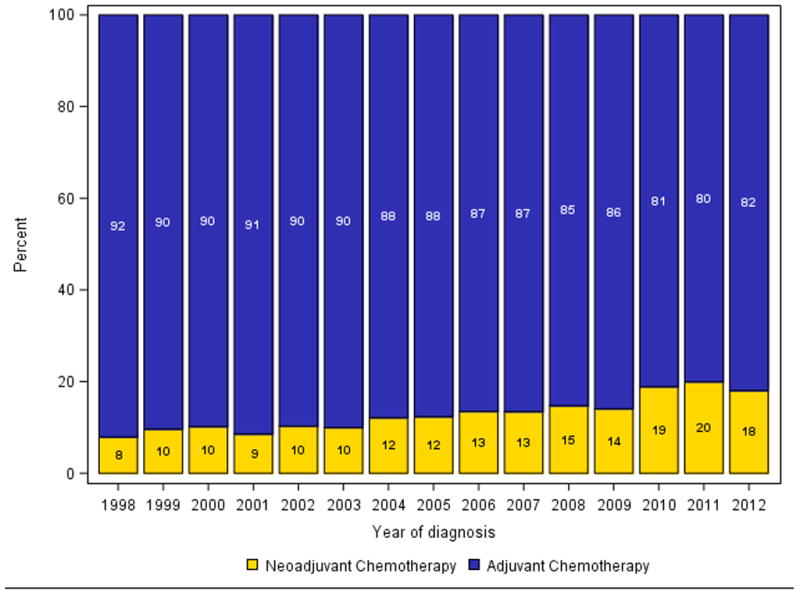
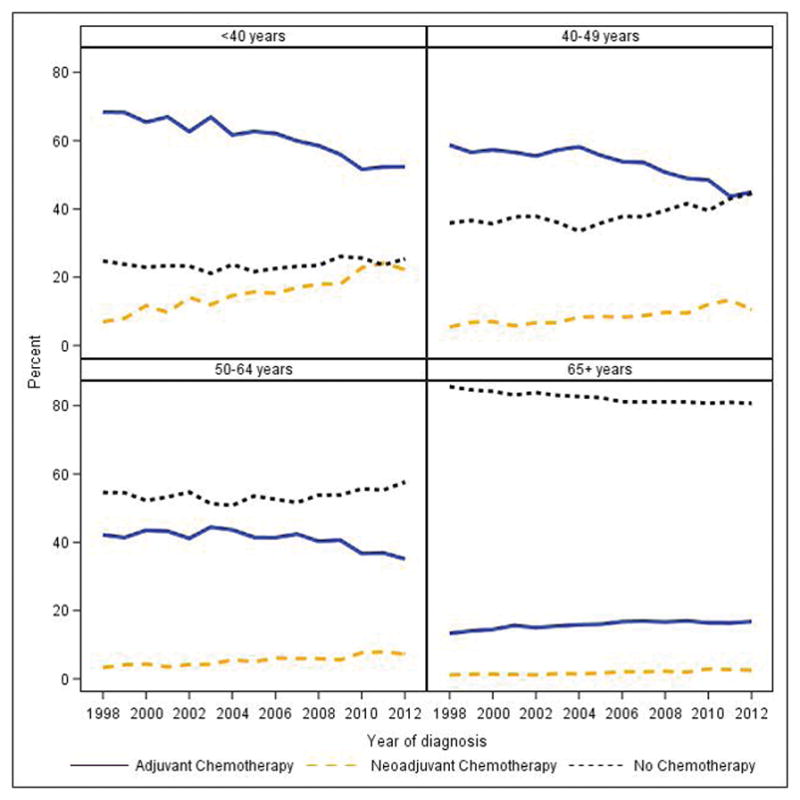
40.1% (94,980) of patients received chemotherapy: 87% (82,588) aCT and 13.0% (12,392) NAC. NAC use more than doubled over time and increased with stage (Stage I, 0.7%; Stage III, 29.9%). Multivariable predictors of NAC treatment were stage (III), younger age (<40 years), Black or Hispanic race/ethnicity [versus non-Hispanic-white, OR 1.10, 95% confidence interval (CI) 1.05–1.16], and care at a National Cancer Institute (NCI)-designated center (OR 1.70, CI 1.58–1.82). Most (68.4%) NAC recipients had mastectomies, and 14.3% of them underwent BLM. In contrast, 47.9% aCT patients had mastectomies with 7.3% BLM. The only independent predictor of BCS after NAC was care at a NCI-designated center (OR 1.28, CI 1.10–1.49), and of BLM, age <40 (vs. 50–64, OR 2.59, CI 2.21–3.03), or residence in the highest socioeconomic neighborhood quintile (vs. lowest, OR 2.10, CI 1.67–2.64).
Conclusion
NAC use remains low. Predictors of surgery type after NAC were sociodemographic rather than clinical, raising concern for disparities in care access.
-
Subjects:
-
Source:Ann Surg. 266(2):353-360.
-
Pubmed ID:27611617
-
Pubmed Central ID:PMC5629002
-
Document Type:
-
Funding:HHSN261201000140C/CA/NCI NIH HHS/United States ; HHSN261201000035C/CA/NCI NIH HHS/United States ; HHSN261201000036C/CA/NCI NIH HHS/United States ; U58 DP000807/DP/NCCDPHP CDC HHS/United States ; HHSN261201000035I/CA/NCI NIH HHS/United States ; HHSN261201000034C/CA/NCI NIH HHS/United States ; U01 CA197282/CA/NCI NIH HHS/United States
-
Volume:266
-
Issue:2
-
Collection(s):
-
Main Document Checksum:urn:sha256:9ed83d42eaaa8e3b0f44be0b75590f3c4516c2afe5f3c41dda44aec2bee37c57
-
Download URL:
-
File Type:
 [PDF
- 592.84 KB
]
[PDF
- 592.84 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access