Survival, Healthcare Utilization, and End-of-life Care among Older Adults with Malignancy-associated Bowel Obstruction: Comparative Study of Surgery, Venting Gastrostomy, or Medical Management
Supporting Files

-
April 2018
-
File Language:
English
Details
-
Alternative Title:Ann Surg
-
Personal Author:
-
Description:Objective
To compare survival, readmissions, and end-of-life care after palliative procedures vs. medical management for malignancy-associated bowel obstruction (MBO).
Background
MBO is a late complication of intra-abdominal malignancy for which surgeons are frequently consulted. Decisions about palliative treatments, which include medical management, surgery, or venting gastrostomy tube (VGT), are hampered by the paucity of outcomes data relevant to patients approaching the end of life.
Methods
Retrospective study using 2001-2012 SEER-Medicare data of patients ≥65 years of age with stage IV ovarian or pancreatic cancer who were hospitalized for MBO. Multivariate competing-risks regression models were used to compare the following outcomes: survival, readmission for MBO, hospice enrollment, ICU care in the last days of life, and location of death in an acute care hospital.
Results
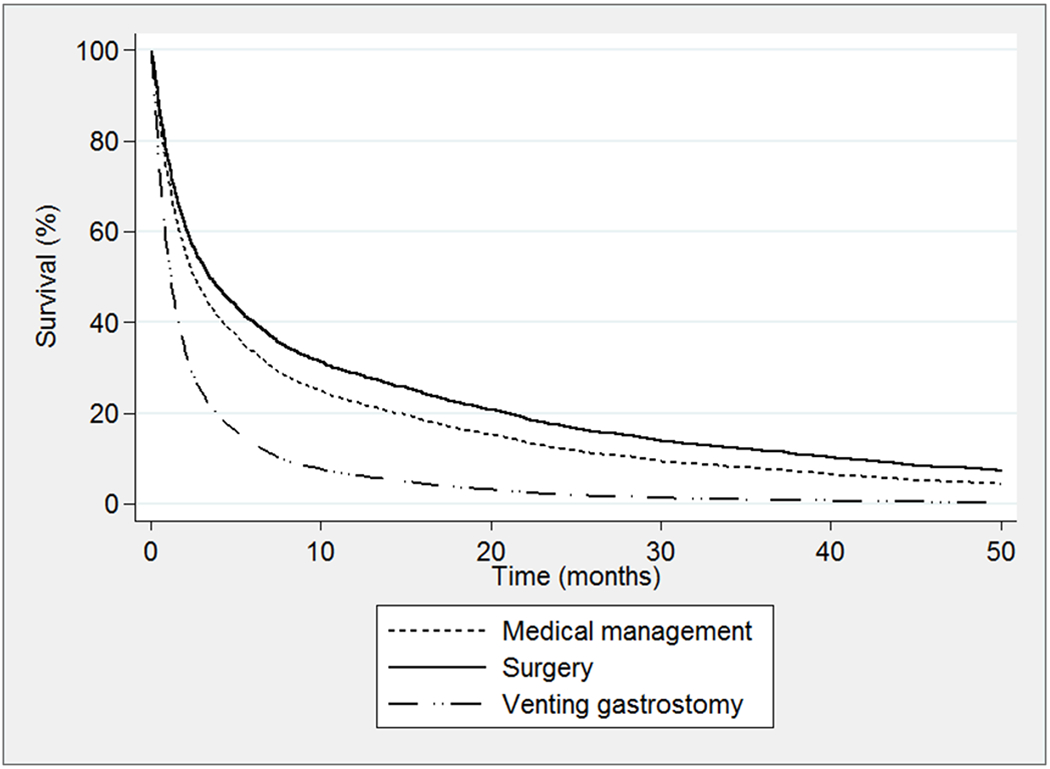
Median survival after MBO admission was 76 days (IQR 26-319 days). Survival was shorter after VGT (38 days [IQR 23-69]) than medical management (72 days [23-312]) or surgery (128 days [42-483]). As compared to medical management, patients treated with VGT had fewer readmissions (subdistribution hazard ratio 0.41[0.29-0.58]), increased hospice enrollment (1.65[1.42-1.91]), and less ICU care (0.69[0.52-0.93]) and in-hospital death (0.47[0.36-0.63]). Surgery was associated with fewer readmissions (0.69[0.59-0.80]), decreased hospice enrollment (0.84[0.76-0.92]), and higher likelihood of ICU care (1.38[1.17-1.64]).
Conclusions
VGT is associated with fewer readmissions and lower intensity healthcare utilization at the end of life than medical management or surgery. Given the limited survival, regardless of management, hospitalization with MBO carries prognostic significance and presents a critical opportunity to identify patients’ priorities for end-of-life care.
-
Subjects:
-
Source:Ann Surg. 267(4):692-699
-
Pubmed ID:28151799
-
Pubmed Central ID:PMC7509894
-
Document Type:
-
Funding:HHSN261201000140C/CA/NCI NIH HHS/United States ; P30 CA008748/CA/NCI NIH HHS/United States ; HHSN261201000035I/CA/NCI NIH HHS/United States ; R25 CA092203/CA/NCI NIH HHS/United States ; U58 DP003862/DP/NCCDPHP CDC HHS/United States ; HHSN261201000035C/PC/NCI NIH HHS/United States ; HHSN261201000034C/CA/NCI NIH HHS/United States
-
Volume:267
-
Issue:4
-
Collection(s):
-
Main Document Checksum:urn:sha256:3994895cfbdb5d31b62f7758d9c1eba6a937c180377587930980957bc180675b
-
Download URL:
-
File Type:
 [PDF
- 600.26 KB
]
[PDF
- 600.26 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access