Outlook for tuberculosis elimination in California: An individual-based stochastic model
Supporting Files
Public Domain

-
April 09 2019
-
File Language:
English
Details
-
Alternative Title:PLoS One
-
Personal Author:
-
Description:Rationale
As part of the End TB Strategy, the World Health Organization calls for low-tuberculosis (TB) incidence settings to achieve pre-elimination (<10 cases per million) and elimination (<1 case per million) by 2035 and 2050, respectively. These targets require testing and treatment for latent tuberculosis infection (LTBI).
Objectives
To estimate the ability and costs of testing and treatment for LTBI to reach pre-elimination and elimination targets in California.
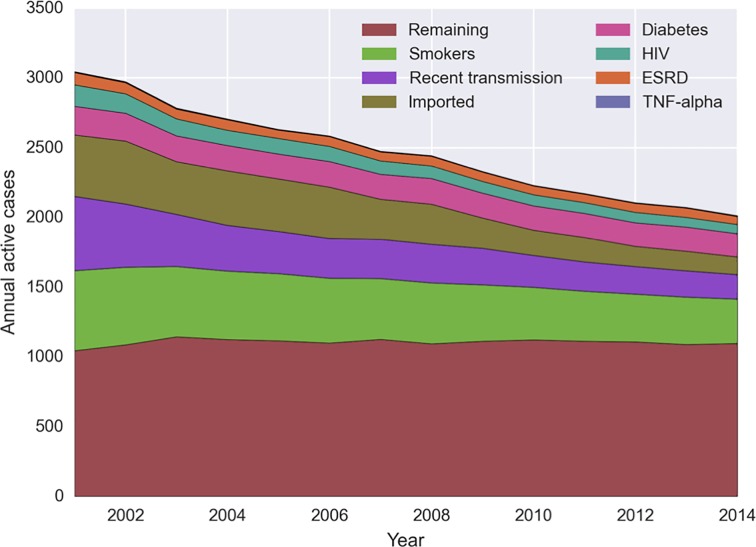
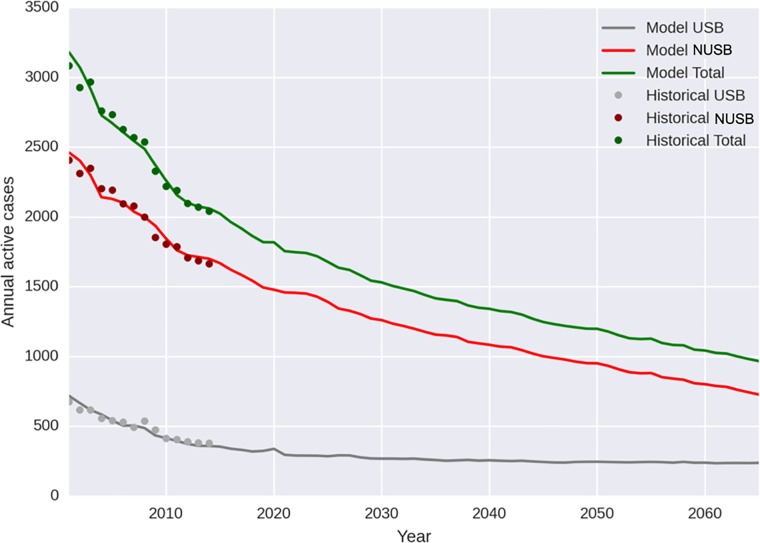
Methods
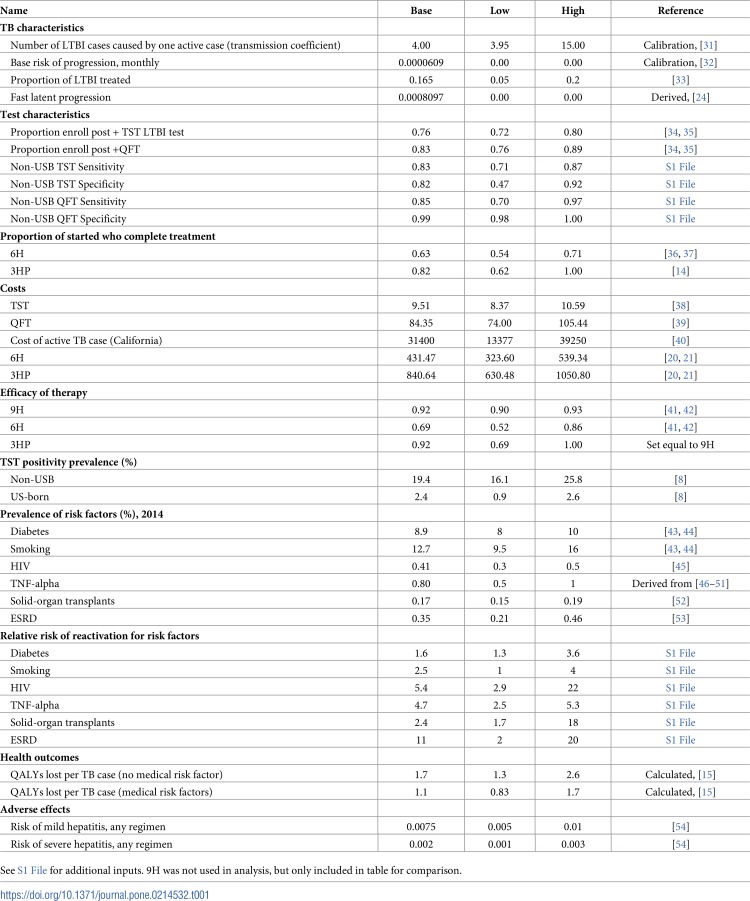
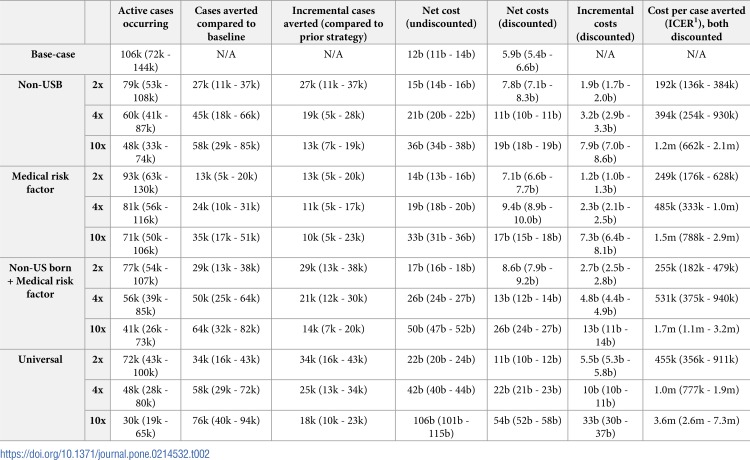
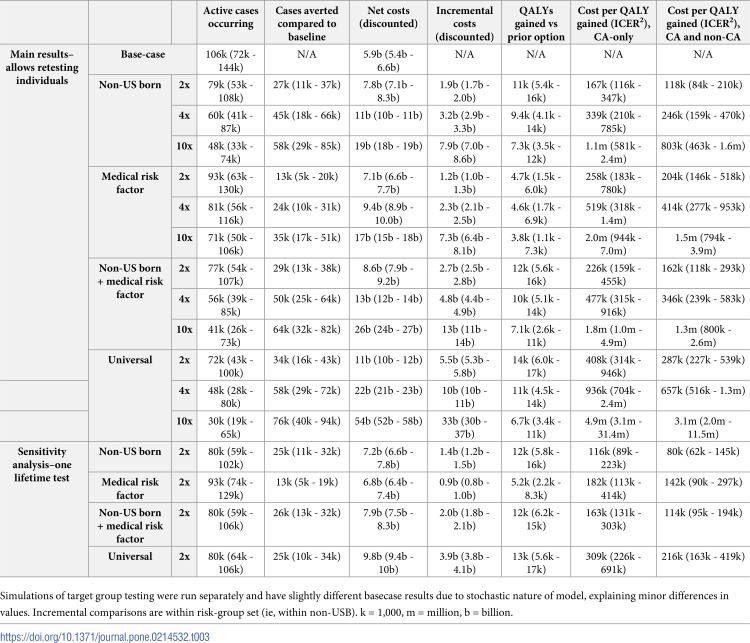
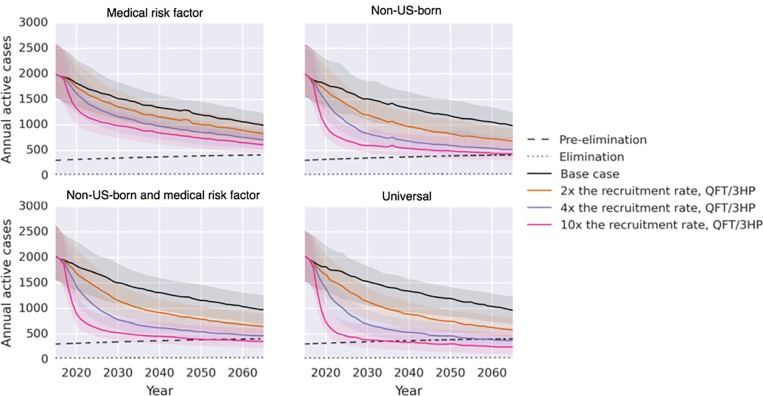
We created an individual-based epidemic model of TB, calibrated to historical cases. We evaluated the effects of increased testing (QuantiFERON-TB Gold) and treatment (three months of isoniazid and rifapentine). We analyzed four test and treat targeting strategies: (1) individuals with medical risk factors (MRF), (2) non-USB, (3) both non-USB and MRF, and (4) all Californians. For each strategy, we estimated the effects of increasing test and treat by a factor of 2, 4, or 10 from the base case. We estimated the number of TB cases occurring and prevented, and net and incremental costs from 2017 to 2065 in 2015 U.S. dollars. Efficacy, costs, adverse events, and treatment dropout were estimated from published data. We estimated the cost per case averted and per quality-adjusted life year (QALY) gained.
Measurements and main results
In the base case, 106,000 TB cases are predicted to 2065. Pre-elimination was achieved by 2065 in three scenarios: a 10-fold increase in the non-USB and persons with MRF (by 2052), and 4- or 10-fold increase in all Californians (by 2058 and 2035, respectively). TB elimination was not achieved by any intervention scenario. The most aggressive strategy, 10-fold in all Californians, achieved a case rate of 8 (95% UI 4–16) per million by 2050. Of scenarios that reached pre-elimination, the incremental net cost was $20 billion (non-USB and MRF) to $48 billion. These had an incremental cost per QALY of $657,000 to $3.1 million. A more efficient but somewhat less effective single-lifetime test strategy reached as low as $80,000 per QALY.
Conclusions
Substantial gains can be made in TB control in coming years by scaling-up current testing and treatment in non-USB and those with medical risks.
-
Subjects:
-
Source:PLoS One. 14(4)
-
Pubmed ID:30964878
-
Pubmed Central ID:PMC6456190
-
Document Type:
-
Name as Subject:
-
Place as Subject:
-
Volume:14
-
Issue:4
-
Collection(s):
-
Main Document Checksum:urn:sha256:ea9a1c5b603217426902f8983732321f359b28bb535ba5919b09a357d7cca05d
-
Download URL:
-
File Type:
 [PDF
- 953.03 KB
]
[PDF
- 953.03 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access