Cost-effectiveness of Testing and Treatment for Latent Tuberculosis Infection in Residents Born Outside the United States With and Without Medical Comorbidities in a Simulation Model
Supporting Files

-
12 2017
-
File Language:
English
Details
-
Alternative Title:JAMA Intern Med
-
Personal Author:
-
Description:IMPORTANCE
Testing for and treating latent tuberculosis infection (LTBI) is among the main strategies to achieve TB elimination in the United States. The best approach to testing among non-US born residents, particularly those with comorbid conditions, is uncertain.
OBJECTIVE
To estimate health outcomes, costs, and cost-effectiveness of LTBI testing and treatment among non-US born residents with and without medical comorbidities.
DESIGN, SETTING, AND PARTICIPANTS
Decision analytic tree and Markov cohort simulation model among non-US born residents with no comorbidities, with diabetes, with HIV infection, or with end-stage renal disease (ESRD) using a health care sector perspective with 3% annual discounting. Strategies compared included no testing, tuberculin skin test (TST), interferon gamma release assay (IGRA), confirm positive (initial TST, IGRA only for TST-positive results; both tests positive indicates LTBI), and confirm negative (initial IGRA, then TST for IGRA-negative; any test positive indicates LTBI). All strategies were coupled to treatment with 3 months of self-administered rifapentine and isoniazid.
MAIN OUTCOMES AND MEASURES
Number needed to test and treat to prevent 1 case of TB reactivation, discounted quality-adjusted life-years (QALYs), discounted lifetime medical costs, and incremental cost-effectiveness ratios (ICERs).
RESULTS
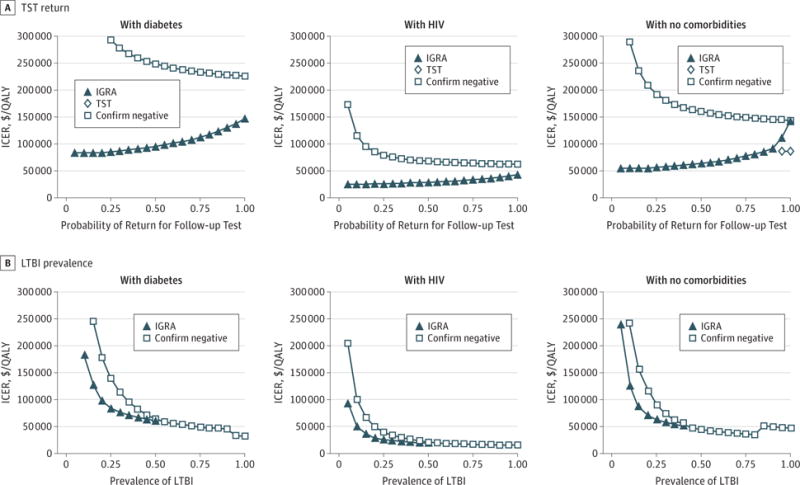
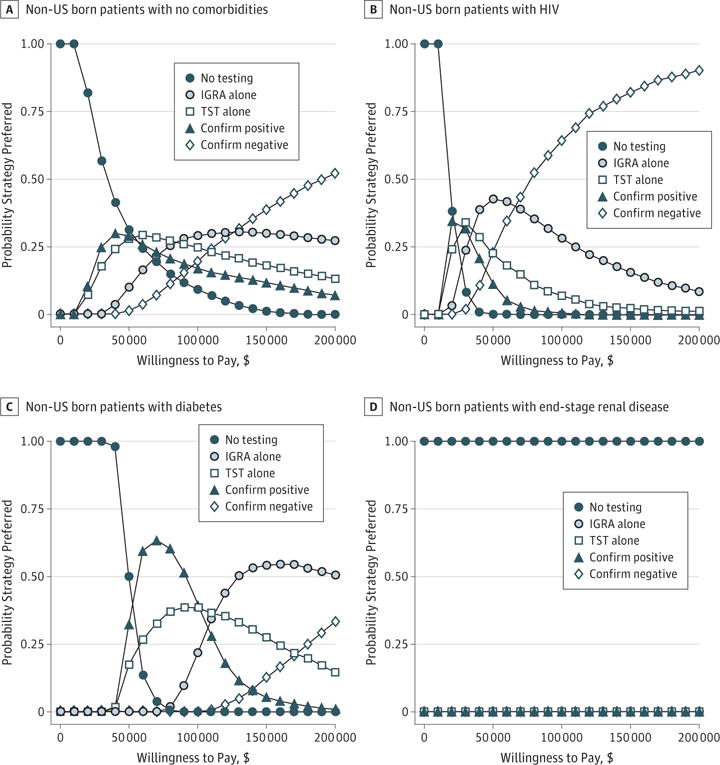
Improving health outcomes increased costs, with choice of test dependent on willingness to pay. Strategies ranked by ascending costs and benefits: no testing, confirm positive, TST, IGRA, and confirm negative. The ICERs varied by non–US born patient risk group: patients with no comorbidities, IGRA was likely cost-effective at $83 000/QALY; patients with diabetes, both confirm positive ($53 000/QALY) and IGRA ($120 000/QALY) were likely cost-effective; patients with HIV, confirm negative was clearly preferred ($63 000/QALY); and patients with ESRD, no testing was cost-effective. Increased LTBI prevalence and reduced return for TST reading improved IGRA’s relative performance. In 10 000 probabilistic simulations among non-US born patients with no comorbidities, with diabetes, and with HIV, some form of testing was virtually always cost-effective. These simulations highlight the uncertainty of test choice for non-US born patients with no comorbidities and non-US born patients with diabetes, but strategies including IGRA were preferred in over 60% of simulations for all non–US born populations except those with ESRD.
CONCLUSIONS AND RELEVANCE
Testing for and treating LTBI among non-US born residents with and without selected comorbidities is likely cost-effective except among those with ESRD in whom competing risks of death limit benefits. Strategies including IGRA fell below a $100 000/QALY willingness-to-pay threshold for non-US born patients with no comorbidities, patients with diabetes, and patients with HIV.
-
Keywords:
-
Source:JAMA Intern Med. 177(12):1755-1764
-
Pubmed ID:29049814
-
Pubmed Central ID:PMC5808933
-
Document Type:
-
Funding:
-
Volume:177
-
Issue:12
-
Collection(s):
-
Main Document Checksum:urn:sha256:f38fdf410c80b9dc59c37dadf02714e341942e964c8f8451aba301e13c890bbc
-
Download URL:
-
File Type:
 [PDF
- 347.16 KB
]
[PDF
- 347.16 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access