Underascertainment of Acute HCV Infections Underascertainment of Acute Hepatitis C Virus Infections in the U.S. Surveillance System A Case Series and Chart Review
Supporting Files

-
8 18 2015
-
File Language:
English
Details
-
Alternative Title:Ann Intern Med
-
Personal Author:
-
Description:Background
In 2010, the incidence of hepatitis C virus (HCV) infection in the United States was estimated to be 17 000 cases annually, based on 850 acute HCV cases reported to the Centers for Disease Control and Prevention by local public health authorities. Absence of symptomatic disease and lack of a specific laboratory test for acute infection complicates diagnosis and surveillance.
Objective
To validate estimates of the incidence of acute HCV infection by determining the reporting rate of clinical diagnoses of acute infection to the Massachusetts Department of Public Health (MDPH) and Centers for Disease Control and Prevention.
Design
Case series and chart review.
Setting
Two hospitals and the state correctional health care system in Massachusetts.
Patients
183 patients clinically diagnosed with acute HCV infection from 2001 to 2011 and participating in a research study.
Measurements
Rate of electronic case reporting of acute HCV infection to the MDPH and rate of subsequent confirmation according to national case definitions.
Results
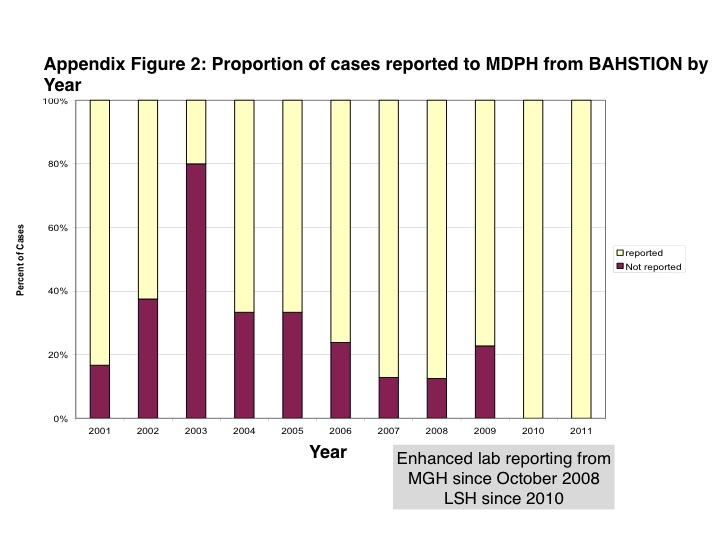
149 of 183 (81.4%) clinical cases of acute HCV infection were reported to the MDPH for surveillance classification. The MDPH investigated 43 of these reports as potential acute cases of HCV infection based on their surveillance requirements; ultimately, only 1 met the national case definition and was counted in nationwide statistics published by the Centers for Disease Control and Prevention. Discordance in clinical and surveillance classification was often related to missing clinical or laboratory data at the MDPH as well as restrictive definitions, including requirements for negative hepatitis A and B laboratory results.
Limitation
Findings may not apply to other jurisdictions because of differences in resources for surveillance.
Conclusion
Clinical diagnoses of acute HCV infection were grossly underascertained by formal surveillance reporting. Incomplete clinician reporting, problematic case definitions, limitations of diagnostic testing, and imperfect data capture remain major limitations to accurate case ascertainment despite automated electronic laboratory reporting. These findings may have implications for national estimates of the incidence of HCV infection.
-
Keywords:
-
Source:Ann Intern Med. 163(4):254-261
-
Pubmed ID:26121304
-
Pubmed Central ID:PMC4731032
-
Document Type:
-
Funding:
-
Volume:163
-
Issue:4
-
Collection(s):
-
Main Document Checksum:urn:sha256:79c4b17ecff38a4ccd234c774d693e91fbad1fd2fc317116357ee668f8edf621
-
Download URL:
-
File Type:
 [PDF
- 365.54 KB
]
[PDF
- 365.54 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access