Access to HIV Viral Load Testing and Antiretroviral Therapy Switch Practices: A Multicountry Prospective Cohort Study in Sub-Saharan Africa
Supporting Files

-
11 2020
-
File Language:
English
Details
-
Alternative Title:AIDS Res Hum Retroviruses
-
Personal Author:
-
Corporate Authors:
-
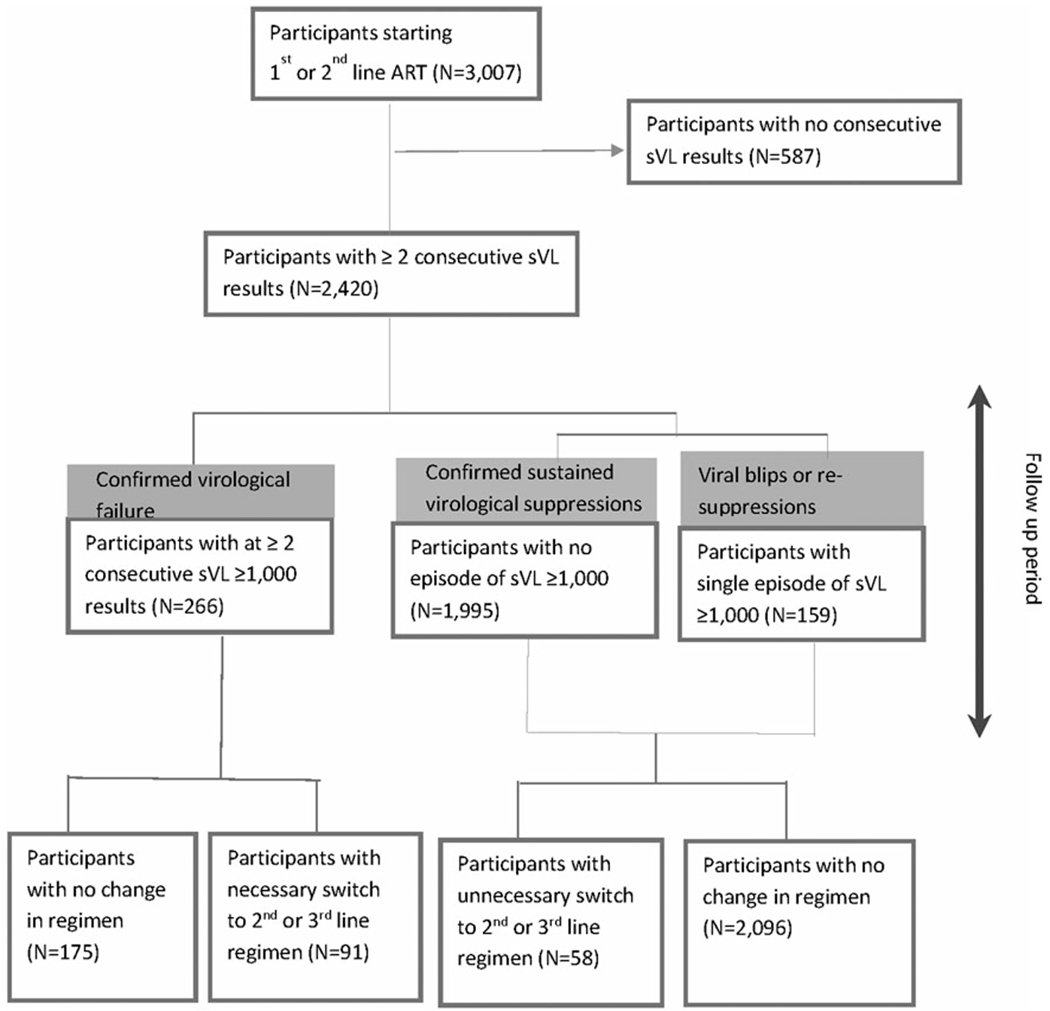
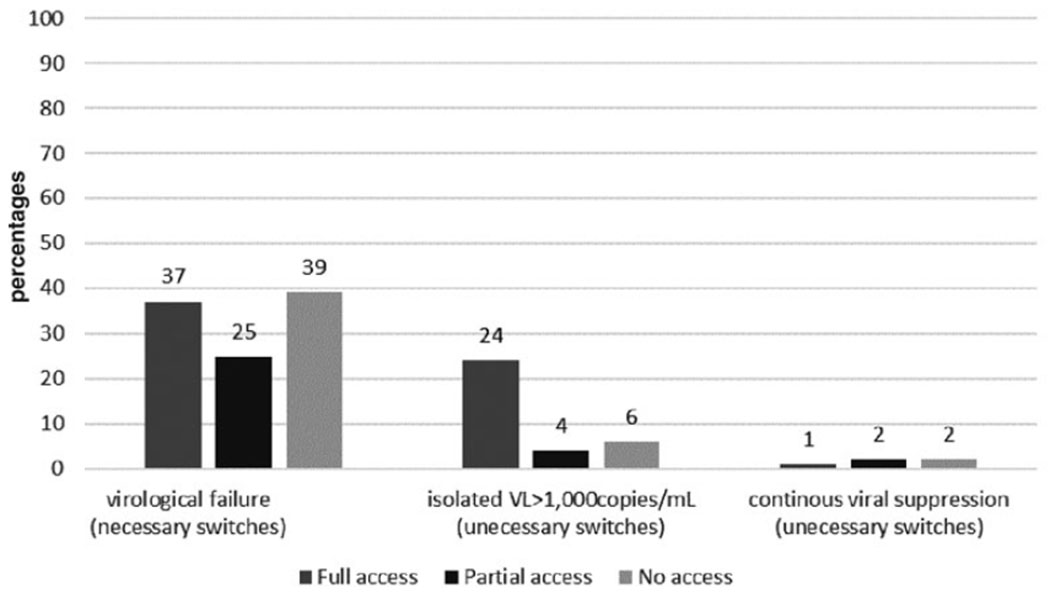
Description:Poor access to HIV viral load (VL) testing prevents the timely monitoring of HIV treatment adherence and efficacy. Factors enabling clinical benefits of VL testing when added to local standards of care, can inform the development of more cost-effective routine VL scale-up plans. We compared antiretroviral therapy (ART) switch practices in 13 clinics across 6 countries, with full (| = 8), phasing-in (| = 3) or no onsite access (| = 2) to VL. The analysis used data from the Pan-African Studies to Evaluate Resistance (PASER), observing virological and drug resistance outcomes among adults receiving first- or second-line ART between 2008 and 2015. Study plasma viral load (sVL) determined at baseline, every 12 months thereafter and at the time of switch served for retrospectively validating switch decisions, categorized into "necessary," "unnecessary," and "missed." Virological failure was defined as two consecutive sVL ≥1,000 HIV-RNA copies/mL. One thousand nine hundred ninety-five of the 2,420 (82.4%) study participants had continuous virological suppression during the median 30 months of follow-up. Among the 266 virological failures (11.0%), the proportion of necessary switches were similar in clinics with full (37%), phasing-in (25%), or no access (39%) to local VL testing. Documented utilization of local VL results for the switch decision was associated with higher percentage of necessary switch (87.6% vs. 67.9%). Shorter time to necessary switch was associated with higher rates of long-term virological suppression, regardless of access to local viral load. Availability of HIV VL testing capacity does not systematically result in adequate switch practices or better virological outcomes. Systems supporting sufficient test demand execution, and actual utilization of results for patient management need strengthening.
-
Subjects:
-
Keywords:
-
Source:AIDS Res Hum Retroviruses. 36(11):918-926
-
Pubmed ID:32722958
-
Pubmed Central ID:PMC7709893
-
Document Type:
-
Funding:
-
Volume:36
-
Issue:11
-
Collection(s):
-
Main Document Checksum:urn:sha256:7bc6e7f9e857f54f2cfc2c3ebfce9653dcafdf996d0c427a1f1aa9d01b3de301
-
Download URL:
-
File Type:
 [PDF
- 248.84 KB
]
[PDF
- 248.84 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access