Eligibility for a Shorter Treatment Regimen for Multidrug-resistant Tuberculosis in the United States, 2011–2016
Supporting Files

-
Feb 14 2020
-
File Language:
English
Details
-
Alternative Title:Clin Infect Dis
-
Personal Author:
-
Description:Background.
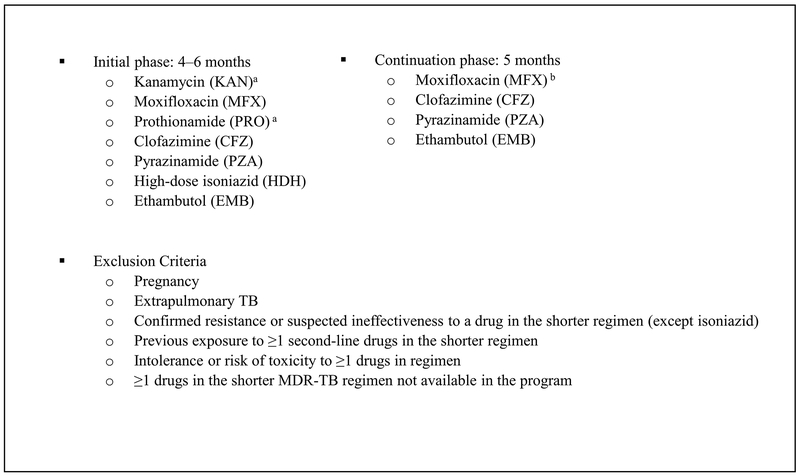
In 2016, the World Health Organization (WHO) recommended a shorter (9–12 month) multidrug-resistant tuberculosis (MDR-TB) treatment regimen (as compared to the conventional 18–24 month regimen) for patients without extrapulmonary TB, pregnancy, previous second-line TB medication exposure, or drug resistance to pyrazinamide, ethambutol, kanamycin, moxifloxacin, ethionamide, or clofazimine. The recommendation was based on successful clinical trials conducted in Asia and Africa, but studies, using mainly European data, have shown few patients in higher resource settings would meet WHO eligibility criteria.
Methods.
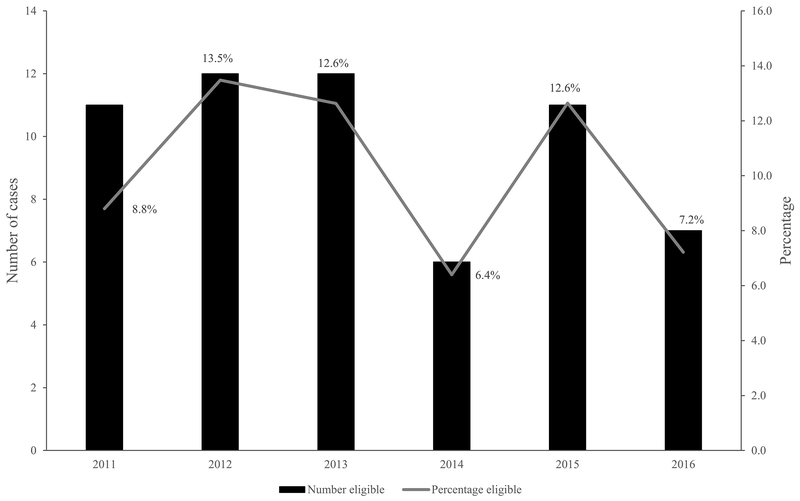
We assessed eligibility for the shorter regimen among U.S. MDR-TB cases that had full drug susceptibility testing (DST) results and were reported during 2011–2016 to the U.S. National TB Surveillance System. We estimated costs by applying the eligibility criteria for the shorter regimen, and proportional inpatient/outpatient costs from a previous population-based study to all MDR-TB patients reported to NTSS.
Results.
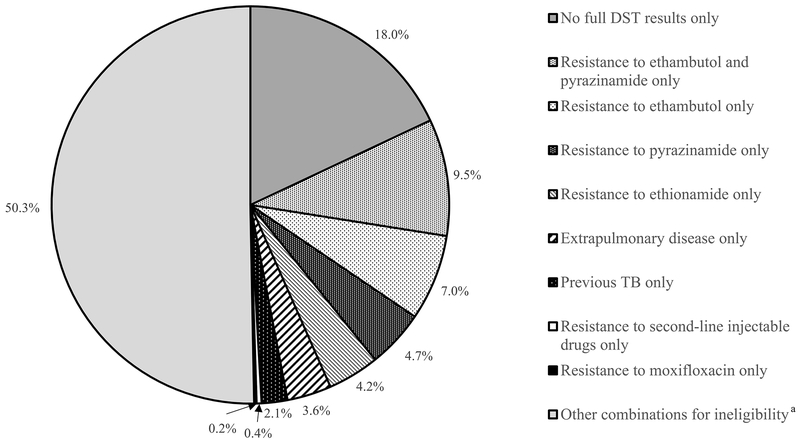
Of 586 reported MDR cases, 10% (59) were eligible for the shorter regimen. Of 527 ineligible patients, 386 had full DST, of which 246 were resistant to ethambutol and 217 resistant to pyrazinamide. Compared with conventional MDR-TB treatment, implementing the shorter regimen would reduce the U.S. annual societal MDR-TB cost burden by 4%, but the cost burden for eligible individuals would be reduced by 37–46%.
Conclusions.
Relying on full DST use, our analysis found a minority of U.S. MDR-TB patients would be eligible for the shorter regimen. Cost reductions would be minimal for society, but large for eligible individuals.
-
Subjects:
-
Source:Clin Infect Dis.
-
Pubmed ID:30944927
-
Pubmed Central ID:PMC6788947
-
Document Type:
-
Funding:
-
Collection(s):
-
Main Document Checksum:urn:sha256:bfe6736af378f5caaa0cffe39a7f6ab7aea2ff3cbae478204857a4213726916b
-
Download URL:
-
File Type:
 [PDF
- 845.54 KB
]
[PDF
- 845.54 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access