Immunogenicity of full and fractional dose of inactivated poliovirus vaccine for use in routine immunization and outbreak response: an open-label, randomized controlled trial
Supporting Files

-
May 16 2019
-
File Language:
English
Details
-
Journal Article:Lancet
-
Personal Author:
-
Description:Background
Intradermal administration of fractional inactivated poliovirus vaccine (fIPV) is a dose-sparing alternative to intramuscular full dose. We assessed the recommendation of two fIPV doses or one IPV dose for routine immunization, and a fIPV booster dose for outbreak response.
Methods
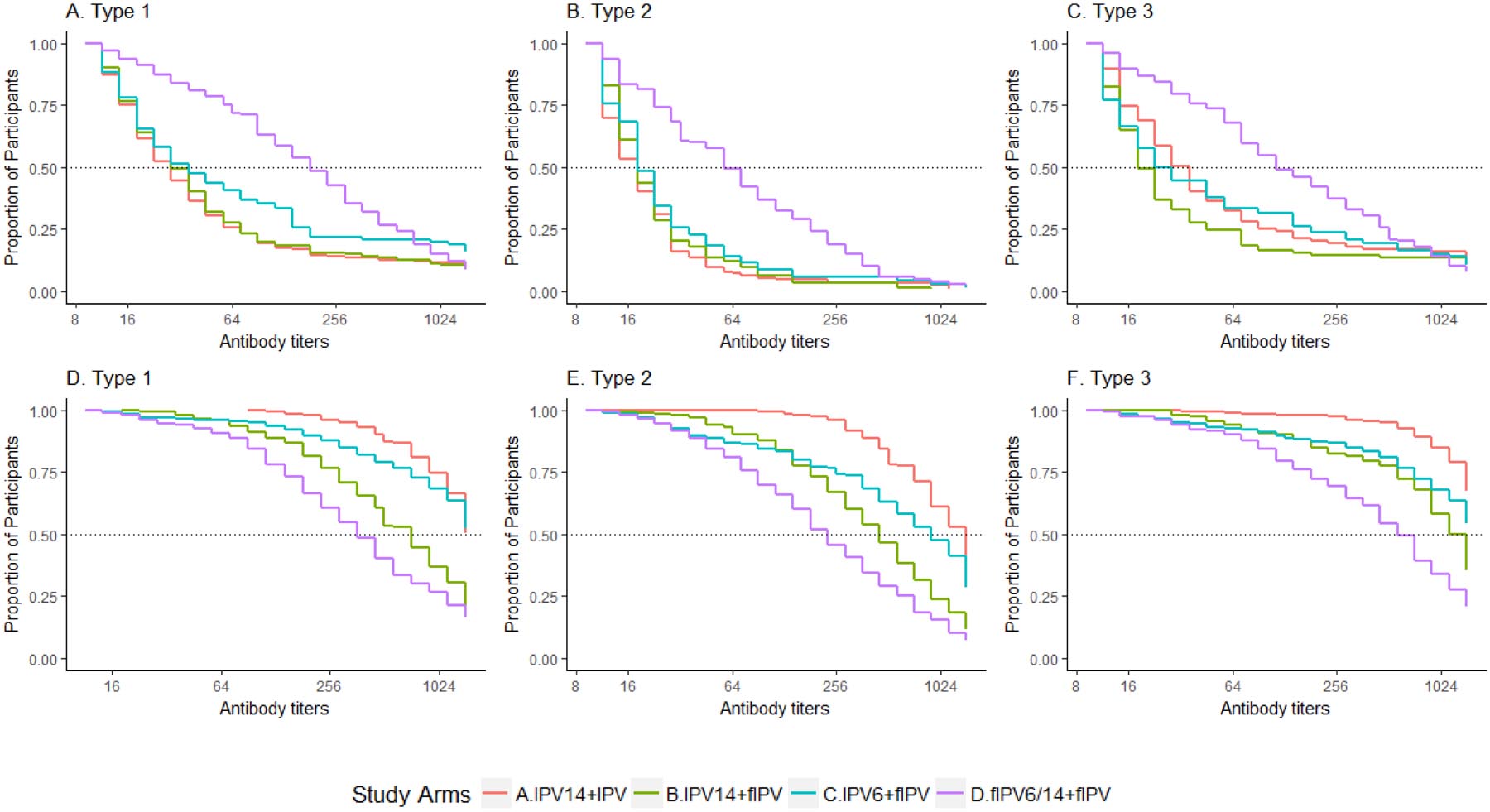
We conducted an open-label, randomized, controlled, inequality, non-inferiority trial in two Dhaka clinics, Bangladesh. Healthy infants were randomized at 6 weeks to one of four arms: (A) IPV at 14 weeks and IPV at 22 weeks (booster); (B) IPV at 14 weeks and fIPV booster; (C) IPV at 6 weeks and fIPV booster; or (D) fIPV at 6+14 weeks and fIPV booster. Vaccines were administered by needle-syringe, with intradermal adapter for fIPV. Vaccine response (seroconversion from seronegative (<1:8) at baseline to seropositive (≥1:8) or four-fold increase in reciprocal antibody titers adjusted for maternal antibody decay) to types 1, 2, and 3 at 22 weeks (routine immunization) and 26 weeks (outbreak response) was assessed in the intention-to-treat population. Non-inferiority margin was 12·5%. (Registered at ClinicalTrials.gov, number NCT02847026).
Findings
From September 1, 2016 to May 2, 2017, 1,076 participants were assigned to Arms A (n=271), B (n=267), C (n=268), and D (n=270). Vaccine response at 22 weeks to two doses of fIPV was significantly higher (p<0.0001) than one dose of IPV (Arm D versus A/B) for type 1 [212 (79%, 95%CI: 73%−83%) versus 305 (57%, 95%CI: 53%−61%)], type 2 [173 (64%, 95%CI: 58%−70%) versus 249 (46%, 95%CI: 42%−51%)], and type 3 [196 (73%, 95%CI: 67%−78%) versus 196 (36%, 95%CI: 33%−41%)]. At 26 weeks, fIPV booster was non-inferior to IPV (Arm B versus A) to types 1 (−1·1%, 90%CI: −2·2% - −0·1%), type 2 (0·4%, 90%CI: −2·2% - 1·4%), and type 3 (−1·5%, 90%CI: −3·2% - −0·2%). Of 129 adverse events, 21 were serious including one death; none were attributed to IPV/fIPV.
Interpretation
fIPV is an effective dose-sparing strategy for routine immunization and outbreak response.
Funding
U.S. Centers for Disease Control and Prevention
-
Subjects:
-
Source:Lancet. 393(10191):2624-2634
-
DOI:
-
Pubmed ID:31104832
-
Pubmed Central ID:PMC7069654
-
Document Type:
-
Funding:
-
Genre:
-
Volume:393
-
Issue:10191
-
Collection(s):
-
Main Document Checksum:urn:sha-512:5e17795479ec7d6560e3a8d7f4706ab30dbb510aed624a177d20499f72522cccce74651356b871bb97b1afd73a2d7bcbe205ab1ba2da4a3f6b88a1d2d22a16d7
-
Download URL:
-
File Type:
 [PDF
- 782.62 KB
]
[PDF
- 782.62 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access