Assessing Variability in Hospital-Level Mortality among U.S. Medicare Beneficiaries with Hospitalizations for Severe Sepsis and Septic Shock
Supporting Files

-
November 2018
-
File Language:
English
Details
-
Alternative Title:Crit Care Med
-
Personal Author:
-
Description:Objective
To assess the variability in short term sepsis mortality by hospital among Centers for Medicare and Medicaid Services beneficiaries in the United States during 2013–2014.
Design
A retrospective cohort design
Setting
Hospitalizations from 3,068 acute care hospitals that participated in the Centers for Medicare and Medicaid Services inpatient prospective payment system in 2013 and 2014.
Patients
Medicare fee-for-service beneficiaries greater than or equal to 65 years old who had an inpatient hospitalization coded with present at admission severe sepsis or septic shock.
Interventions
None.
Measurements, Main Results
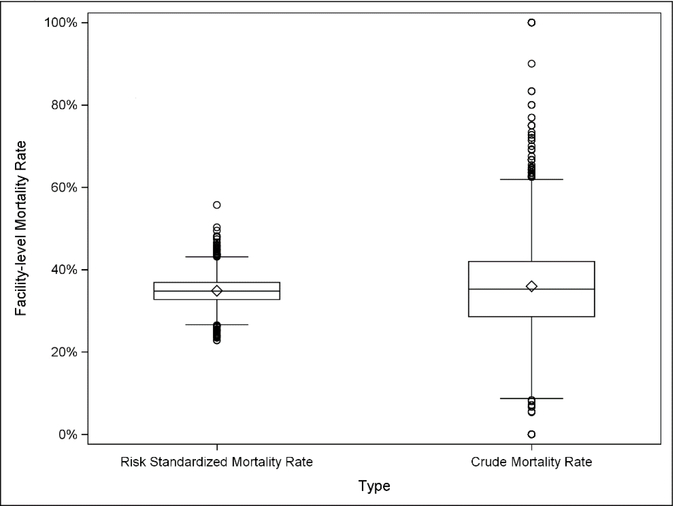
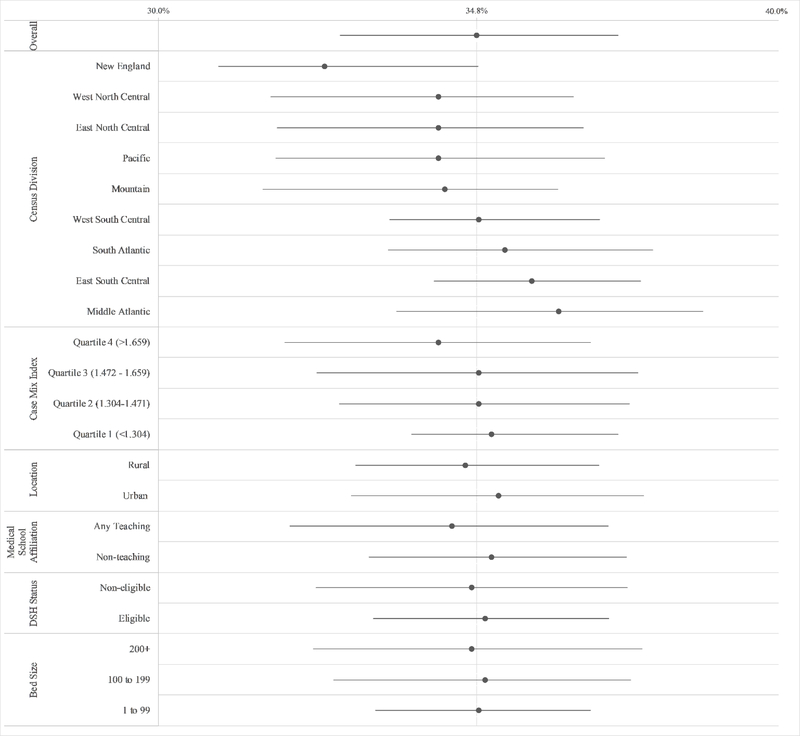
Individual level mortality was assessed as death at or within 7 days of hospital discharge and aggregated to calculate hospital-level mortality rates. We used a logistic hierarchal linear model to calculate mortality risk-adjusted for patient characteristics. We quantified variability among hospitals using the median odds ratio (MOR), and calculated risk-standardized mortality rates (risk-standardized mortality rates) for each hospital. The overall crude mortality rate was 34.7%. We found significant variability in mortality by hospital (p<0.001). The middle 50% of hospitals had similar risk-standardized mortality rates (32.7–36.9%), whereas the decile of hospitals with the highest risk-standardized mortality rates had a median mortality rate of 40.7%, compared to a median of 29.2% for hospitals in the decile with the lowest risk-standardized mortality rates. The median odds ratio (1.29) was lower than the adjusted odds ratios for several measures of patient comorbidities and severity of illness, including present at admission organ dysfunction, no identified source of infection, and age.
Conclusions
In a large study of present at admission sepsis among Medicare beneficiaries, we showed that mortality was most strongly associated with underlying comorbidities and measures of illness on arrival. However, after adjusting for patient characteristics, mortality also modestly depended on where a patient with sepsis received care, suggesting that efforts to improve sepsis outcomes in lower performing hospitals could impact sepsis survival.
-
Subjects:
-
Source:Crit Care Med. 46(11):1753-1760
-
Pubmed ID:30024430
-
Pubmed Central ID:PMC6774245
-
Document Type:
-
Funding:
-
Place as Subject:
-
Volume:46
-
Issue:11
-
Collection(s):
-
Main Document Checksum:urn:sha256:2b4c4a8e5a459fc88caf6f5a59124a42a3e6b4fd1b733653d81d0ed543511bb8
-
Download URL:
-
File Type:
 [PDF
- 360.62 KB
]
[PDF
- 360.62 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access