High Rate of Treatment Completion in Program Settings with 12-Dose Weekly Isoniazid and Rifapentine (3HP) for Latent Mycobacterium tuberculosis Infection
Supporting Files

-
Oct 01 2017
-
File Language:
English
Details
-
Alternative Title:Clin Infect Dis
-
Personal Author:Sandul, Amy L. ; Nwana, Nwabunie ; Holcombe, J. Mike ; Lobato, Mark N. ; Marks, Suzanne ; Webb, Risa ; Wang, Shu-Hua ; Stewart, Brock ; Griffin, Phil ; Hunt, Garrett ; Shah, Neha ; Marco, Asween ; Patil, Naveen ; Mukasa, Leonard ; Moro, Ruth N. ; Jereb, John ; Mase, Sundari ; Chorba, Terence ; Bamrah-Morris, Sapna ; Ho, Christine S.
-
Description:Background
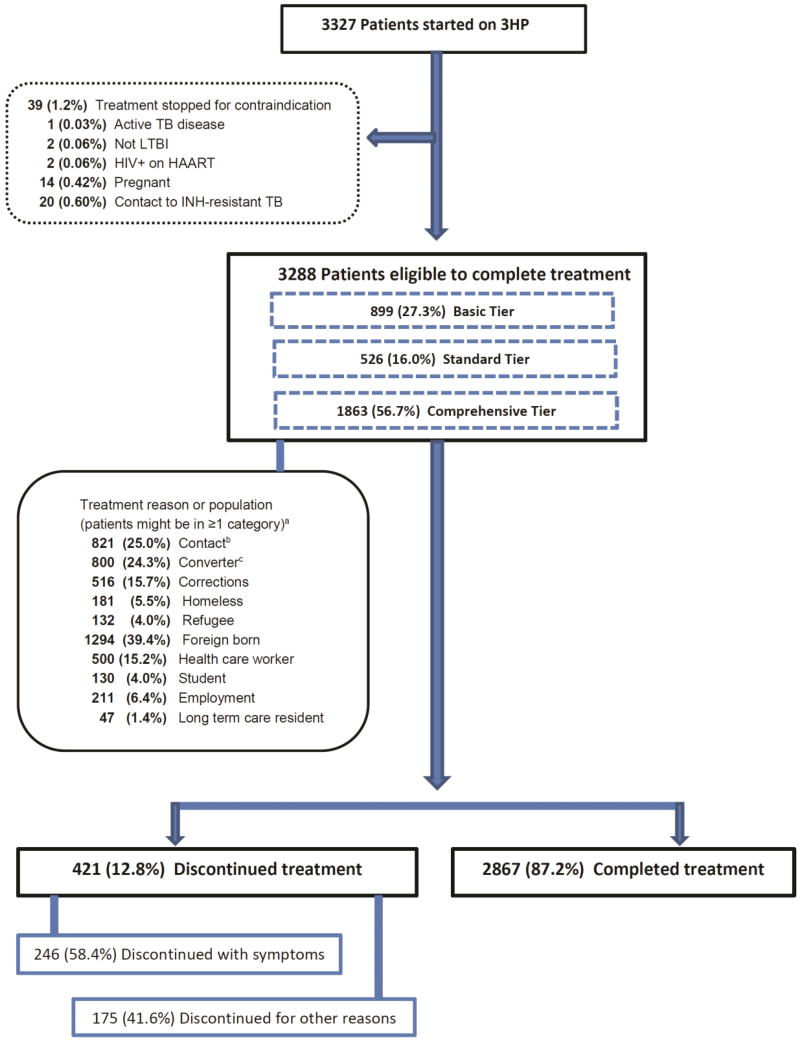
RCTs demonstrated the newest LTBI regimen, 12 weekly doses of directly observed isoniazid and rifapentine (3HP), as efficacious as 9 months of isoniazid (9H) with a greater completion rate (82% versus 69%); however, 3HP has not been assessed in routine health care settings.
Methods
Observational cohort of LTBI patients receiving 3HP through 16 US programs was used to assess treatment completion, adverse drug reactions (ADRs), and factors associated with treatment discontinuation.
Results
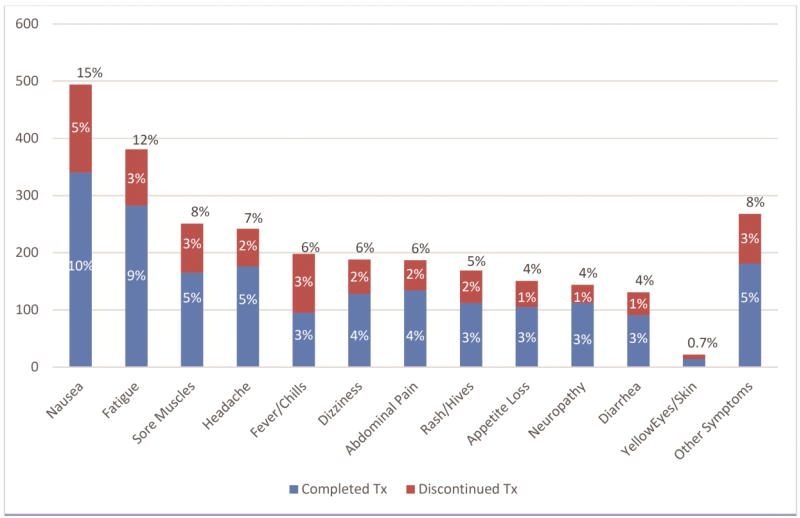
Of 3288 patients eligible to complete 3HP, 2867 (87.2%) completed treatment. Children 2–17 years had the highest completion rate, 94.5% (155/164). Patients reporting homelessness had a completion rate of 81.2% (147/181). In univariable analyses, discontinuation was lowest among children (relative risk [RR], 0.44 [95% CI, 0.23–0.85]; P = .014), and highest in persons ≥65 years (RR, 1.72 [95% CI, 1.25–2.35] P = .001). In multivariable analyses, discontinuation was lowest among contacts of patients with TB disease (adjusted relative risk [ARR], 0.68 [95% CI, 0.52–0.89]; P = .005), and students (ARR, 0.45 [95% CI, 0.21–0.98]; P = .044); highest with incarceration (ARR, 1.43 [95% CI, 1.08–1.89]; P=.013) and homelessness (ARR, 1.72 [95% CI, 1.25–2.39]; P = .001). ADRs were reported by 1174 (35.7%) patients, of whom 891 (76.0%) completed treatment.
Conclusions
Completion of 3HP in routine health care settings was greater overall than rates reported from clinical trials, and greater than historically observed using other regimens among reportedly nonadherent populations. Widespread use of 3HP for LTBI treatment could accelerate elimination of TB disease in the United States.
-
Subjects:
-
Source:Clin Infect Dis. 65(7):1085-1093.
-
Pubmed ID:28575208
-
Pubmed Central ID:PMC5709238
-
Document Type:
-
Funding:
-
Volume:65
-
Issue:7
-
Collection(s):
-
Main Document Checksum:urn:sha256:5f543ca0bb506ebffd457ff1d65d9c2bf0776e45348664f9afc1586c408b35b9
-
Download URL:
-
File Type:
 [PDF
- 621.18 KB
]
[PDF
- 621.18 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access