Cardiovascular Disease Risk Prediction in the HIV Outpatient Study
Supporting Files

-
Sep 09 2016
-
File Language:
English
Details
-
Alternative Title:Clin Infect Dis
-
Personal Author:
-
Description:Background
Cardiovascular disease (CVD) risk prediction tools are often applied to populations beyond those in which they were designed when validated tools for specific subpopulations are unavailable.
Methods
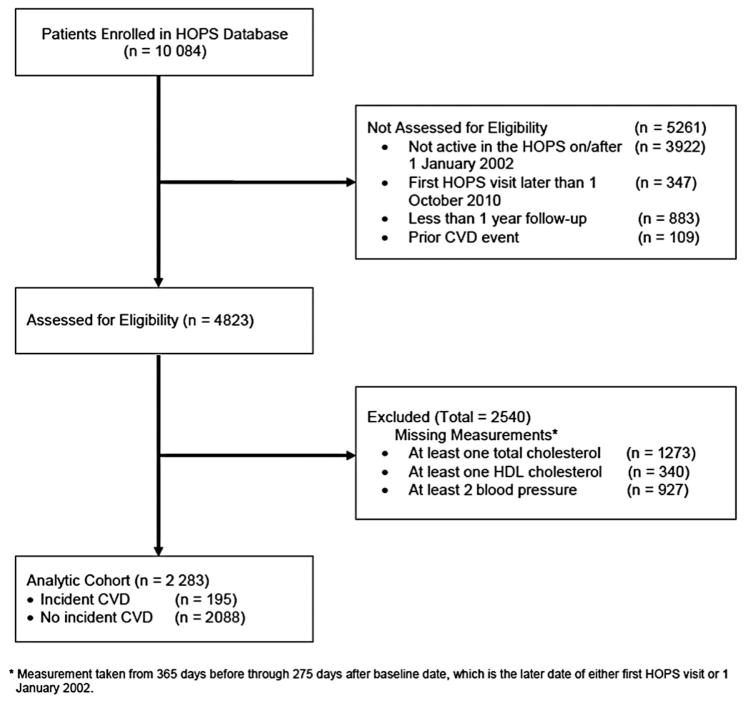
Using data from 2283 human immunodeficiency virus (HIV)–infected adults aged ≥18 years, who were active in the HIV Outpatient Study (HOPS), we assessed performance of 3 commonly used CVD prediction models developed for general populations: Framingham general cardiovascular Risk Score (FRS), American College of Cardiology/American Heart Association Pooled Cohort equations (PCEs), and Systematic COronary Risk Evaluation (SCORE) high-risk equation, and 1 model developed in HIV-infected persons: the Data Collection on Adverse Effects of Anti-HIV Drugs (D:A:D) study equation. C-statistics assessed model discrimination and the ratio of expected to observed events (E/O) and Hosmer-Lemeshow χ2P value assessed calibration.
Results
From January 2002 through September 2013, 195 (8.5%) HOPS participants experienced an incident CVD event in 15 056 person-years. The FRS demonstrated moderate discrimination and was well calibrated (C-statistic: 0.66, E/O: 1.01, P = .89). The PCE and D:A:D risk equations demonstrated good discrimination but were less well calibrated (C-statistics: 0.71 and 0.72 and E/O: 0.88 and 0.80, respectively; P < .001 for both), whereas SCORE performed poorly (C-statistic: 0.59, E/O: 1.72; P = .48).
Conclusions
Only the FRS accurately estimated risk of CVD events, while PCE and D:A:D underestimated risk. Although these models could potentially be used to rank US HIV-infected individuals at higher or lower risk for CVD, the models may fail to identify substantial numbers of HIV-infected persons with elevated CVD risk who could potentially benefit from additional medical treatment.
-
Subjects:
-
Source:Clin Infect Dis. 63(11):1508-1516.
-
Pubmed ID:27613562
-
Pubmed Central ID:PMC5624518
-
Document Type:
-
Funding:
-
Volume:63
-
Issue:11
-
Collection(s):
-
Main Document Checksum:urn:sha256:1b266936c68a25514a75a86efd4d28c62b7976d23f9974f9ca3c9e02809e1221
-
Download URL:
-
File Type:
 [PDF
- 537.56 KB
]
[PDF
- 537.56 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access