Contrasting predictors of poor antiretroviral therapy outcomes in two South African HIV programmes: a cohort study
Supporting Files

-
Jul 22 2010
-
File Language:
English
Details
-
Alternative Title:BMC Public Health
-
Personal Author:
-
Description:Background
Many national antiretroviral therapy (ART) programmes encourage providers to identify and address baseline factors associated with poor treatment outcomes, including modifiable adherence-related behaviours, before initiating ART. However, evidence on such predictors is scarce, and providers judgement may often be inaccurate. To help address this evidence gap, this observational cohort study examined baseline factors potentially predictive of poor treatment outcomes in two ART programmes in South Africa, with a particular focus on determinants of adherence.
Methods
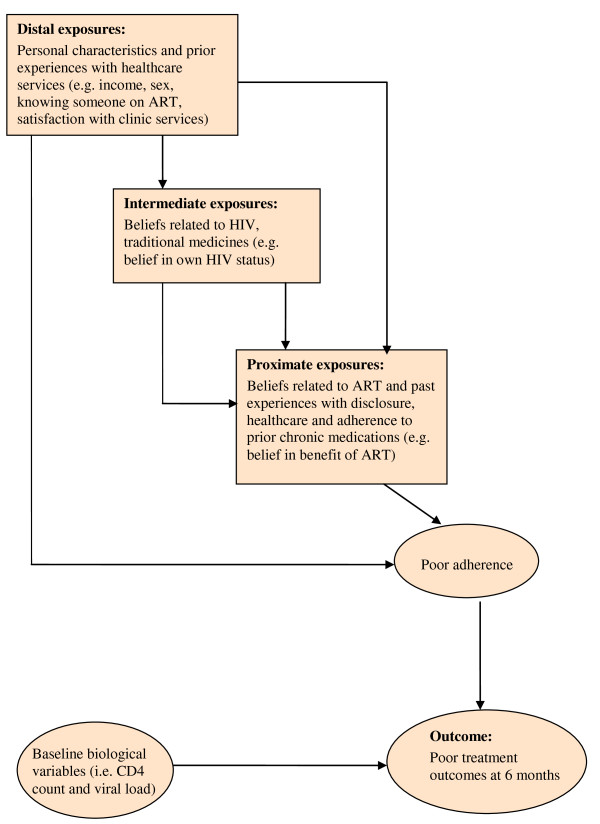
Treatment-naïve patients starting ART were enrolled from a community and a workplace ART programme. Potential baseline predictors associated with poor treatment outcomes (defined as viral load > 400 copies/ml or having discontinued treatment by six months) were assessed using logistic regression. Exposure variables were organised for regression analysis using a hierarchical framework.
Results
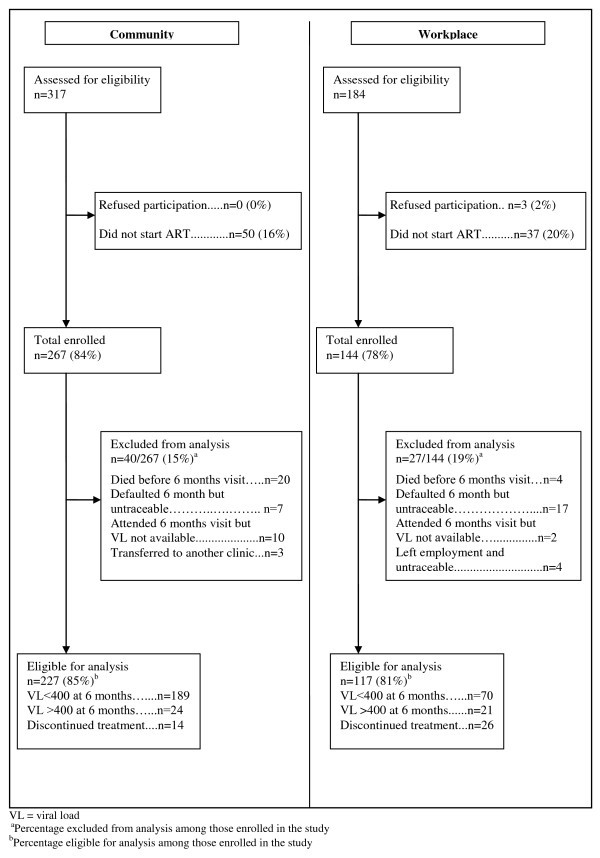
38/227 (17%) of participants in the community had poor treatment outcomes compared to 47/117 (40%) in the workplace. In the community, predictors of worse outcomes included: drinking more than 20 units of alcohol per week, having no prior experience of chronic medications, and consulting a traditional healer in the past year (adjusted odds ratio [aOR] 15.36, 95% CI 3.22-73.27; aOR 2.30, 95%CI 1.00-5.30; aOR 2.27, 95% CI 1.00-5.19 respectively). Being male and knowing someone on ART were associated with better outcomes (aOR 0.25, 95%CI 0.09-0.74; aOR 0.44, 95%CI 0.19-1.01 respectively). In the workplace, predictors of poor treatment outcomes included being uncertain about the health effects of ART and a traditional healer's ability to treat HIV (aOR 7.53, 95%CI 2.02-27.98; aOR 4.40, 95%CI 1.41-13.75 respectively). Longer pre-ART waiting time (2-12 weeks compared to <2 weeks) predicted better treatment outcomes (aOR 0.13, 95% CI 0.03-0.56).
Conclusion
Baseline predictors of poor treatment outcomes were largely unique to each programme, likely reflecting different populations and pathways to HIV care. In the workplace, active promotion of HIV testing may have extended ART to individuals who, without provider initiation, would not have spontaneously sought care. As provider-initiated testing makes ART available to individuals less motivated to seek care, patients may need additional adherence support, especially addressing uncertainty about the health benefits of ART.
-
Subjects:
-
Source:BMC Public Health. 2010; 10:430.
-
Pubmed ID:20649946
-
Pubmed Central ID:PMC2920888
-
Document Type:
-
Funding:
-
Place as Subject:
-
Volume:10
-
Collection(s):
-
Main Document Checksum:urn:sha256:e598800df073f03942b1662c95019a5d52d7927280d00d3f06ef184cce1c84cf
-
Download URL:
-
File Type:
 [PDF
- 481.88 KB
]
[PDF
- 481.88 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like