A Randomized Clinical Trial Evaluating the Management of Pre-Treatment HIV Drug Resistance by Oligonucleotide Ligation Assay
Supporting Files

-
December 07 2019
-
File Language:
English
Details
-
Alternative Title:Lancet HIV
-
Personal Author:
-
Description:Background
Although experts have recommended testing for pretreatment drug resistance (PDR) prior to ART initiation, there is little evidence to support its implementation. Our aim was to determine whether an inexpensive point mutation assay can improve virologic suppression by identifying PDR to guide drug selection for ART in a lower-middle income country.
Methods
Investigators conducted a randomized multicenter clinical trial between May 28, 2013 and February 3, 2016 at three HIV treatment sites across Kenya: two in Nairobi and one in rural Maseno. A total of 991 HIV-infected, ART-eligible participants were enrolled and followed for twelve months after randomization. We randomized participants (1:1) to either to PDR testing by oligonucleotide ligation assay (OLA) to guide selection of ART or to standard-of-care (SOC), which did not include OLA testing. The OLA-guided therapy arm had pre-ART peripheral blood mononuclear cells evaluated for drug resistance to NNRTI at codons K103N, Y181C, G190A, and to lamivudine at M184V, and when ≥1 drug resistant codon was detected in a participant’s pre-ART specimen, clinicians were directed to prescribe protease inhibitor-based second-line ART. Those without detected resistance and those who were randomized to SOC received NNRTI-based first-line ART. The primary outcome was plasma HIV-1 RNA ≥400 copies per µL at 4, 8, or 12 months after ART initiation which defined virologic failure.
Findings
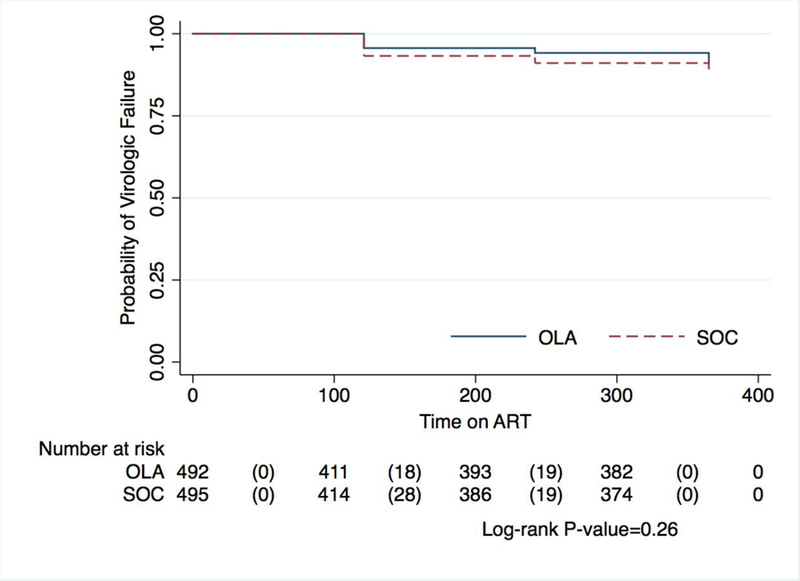
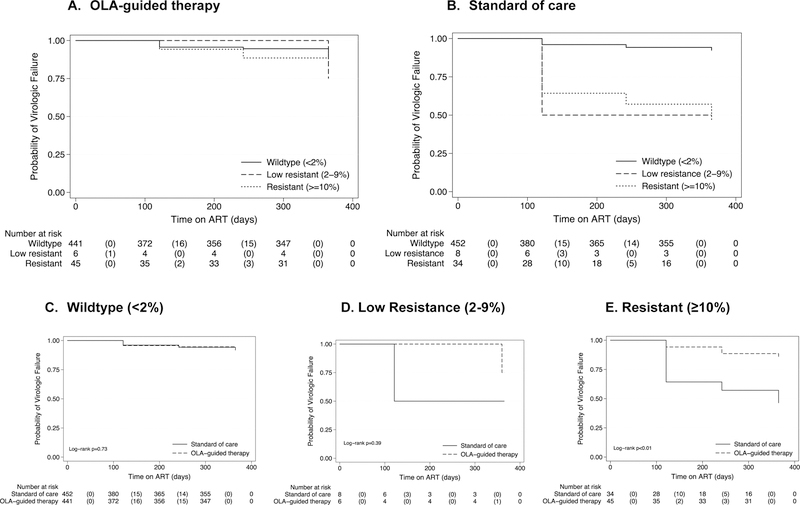
Among the 991 participants randomized to OLA-guided therapy (n=494) and SOC (n=497) the overall PDR prevalence was 9·4% (n=93) [95% confidence interval (CI), 7·7–11·4]. Virologic failure at month-12 of ART in the OLA-guided therapy arm was 8·5% (n=34) [95% CI, 6·0%–11·7%] compared to 9·7% (n=39) (95% CI, 7·0%–13·0%) in SOC and this was not a statistically significant difference (log-rank test, p=0·26). Among participants with PDR, virologic failure was lower in the OLA-guided therapy arm compared to SOC [14% (n=5) vs. 50% (n=13); p<0·01). Among those prescribed NNRTI-based ART, participants given efavirenz were less likely to experience virologic failure compared to those receiving nevirapine [Odds Ratio (OR) = 0·37; 95% CI, 0·22–0·62; p<0·01).
Interpretation
Our finding that OLA testing for PDR reduced virologic failure in only those with specific PDR mutations suggests that PDR poses less of a risk for virologic failure than that predicted by past prevalence estimates, and that the value of PDR testing to reduce virologic failure should be assessed to current antiretroviral treatment regimens.
National Institutes of Health
Trial Status and Registration
The study was completed and is registered with Clinicaltrials.gov #
-
Subjects:
-
Source:Lancet HIV.
-
Pubmed ID:31818716
-
Pubmed Central ID:PMC6936934
-
Document Type:
-
Funding:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:urn:sha256:4facc3c4905f36f7752d8bcd70fd23b7af1377f913e9fdac8ed68e2c5c7b36e1
-
Download URL:
-
File Type:
 [PDF
- 744.97 KB
]
[PDF
- 744.97 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access