Concurrent advanced HIV disease and viral load suppression in a high-burden setting: Findings from the 2015–6 ZIMPHIA survey
Supporting Files
Public Domain

-
June 25 2020
-
File Language:
English
Details
-
Alternative Title:PLoS One
-
Personal Author:
-
Description:Background
As Zimbabwe approaches epidemic control of HIV, programs now prioritize viral load over CD4 monitoring, making it difficult to identify persons living with HIV (PLHIV) suffering from advanced disease (AD). We present an analysis of cross-sectional ZIMPHIA data, highlighting PLHIV with AD and concurrent viral load suppression (VLS).
Methods
ZIMPHIA collected blood specimens for HIV testing from 22,501 consenting adults (ages 15 years and older); 3,466 PLHIV had CD4 and VL results. Household HIV testing used the national serial algorithm, and those testing positive then received point-of-care CD4 enumeration with subsequent VL testing. We used logistic regression analysis to explore factors associated with concurrent AD and VLS (<1000 copies/mL). All analyses were weighted to account for complex survey design.
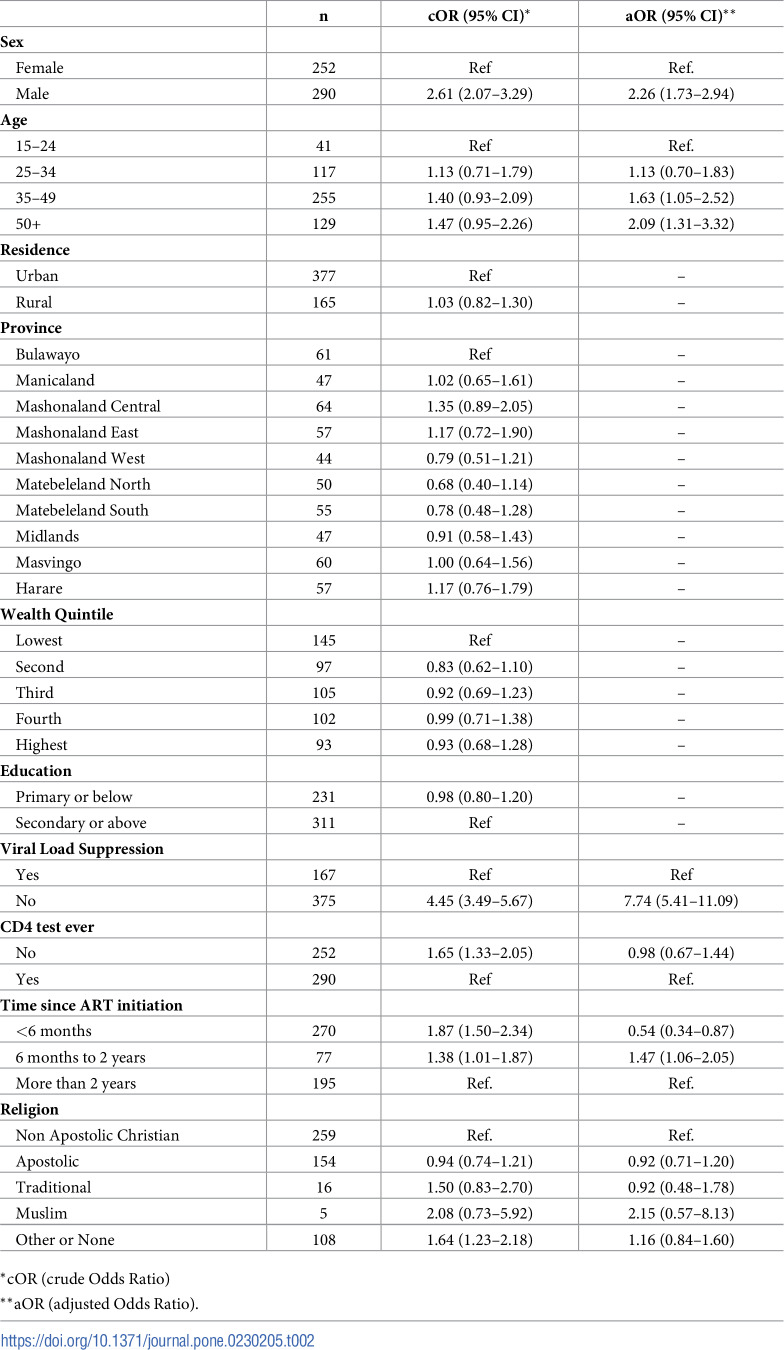
Results
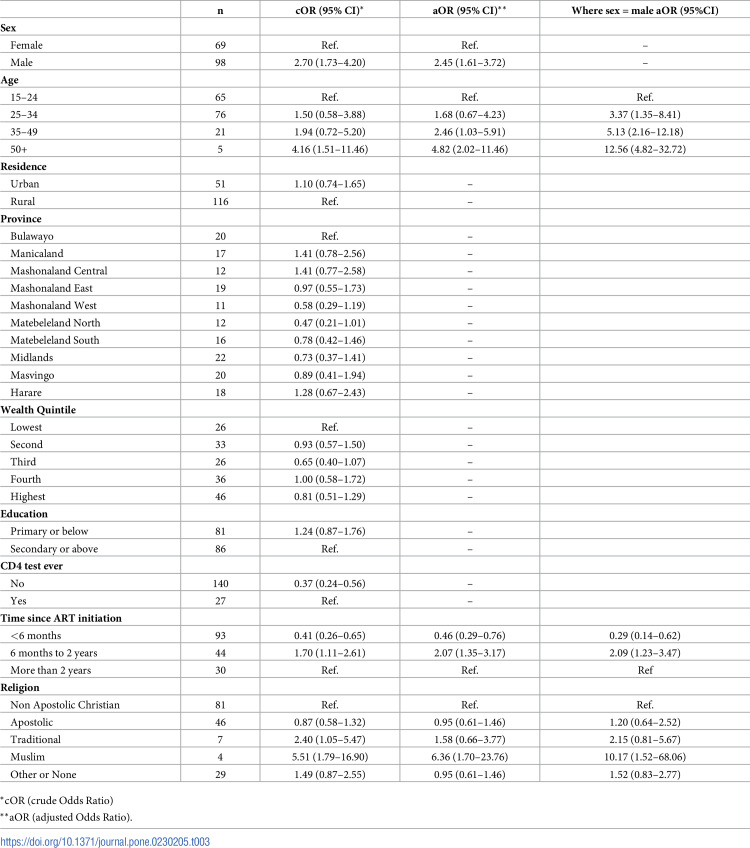
Of the 3,466 PLHIV in the survey with CD4 and VL results, 17% were found to have AD (CD4<200cells/mm3). Of all AD patients, 30% had VLS. Concurrent AD and VLS was associated with male sex (aOR 2.45 95%CI 1.61–3.72), older age (35–49 years [aOR 2.46 95%CI 1.03–5.91] and 50+ years [aOR 4.82 95%CI 2.02–11.46] vs 15–24 years), and ART duration (<6 months [aOR 0.46 95%CI 0.29–0.76] and 6–24 months [aOR 2.07 95%CI 1.35–3.17] vs more than 2 years). The relationship between sex and AD is driven by age with significant associations among men aged 25–34, (aOR 3.37 95%CI 1.35–8.41), 35–49 (aOR 5.13 95%CI 2.16–12.18), and 50+ (aOR 12.56 95%CI 4.82–32.72) versus men aged 15–24.
Conclusions
The percentage of PLHIV with AD and VLS illustrates the conundrum of decreased support for CD4 monitoring, as these patients may not receive appropriate clinical services for advanced HIV disease. In high-prevalence settings such as Zimbabwe, CD4 monitoring support warrants further consideration to differentiate care appropriately for the most vulnerable PLHIV. Males may need to be prioritized, given their over-representation in this sub-population.
-
Subjects:
-
Source:PLoS One. 15(6)
-
Pubmed ID:32584821
-
Pubmed Central ID:PMC7316262
-
Document Type:
-
Place as Subject:
-
Volume:15
-
Issue:6
-
Collection(s):
-
Main Document Checksum:urn:sha256:67bd0e332b25f4e57356f2c409db46b24706dd841fa6294a9eb95e0ed836a264
-
Download URL:
-
File Type:
 [PDF
- 591.87 KB
]
[PDF
- 591.87 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access