Epidemiology of Hospital-Onset versus Community-Onset Sepsis in U.S. Hospitals and Association with Mortality: A Retrospective Analysis Using Electronic Clinical Data
Supporting Files

-
September 2019
-
File Language:
English
Details
-
Alternative Title:Crit Care Med
-
Personal Author:
-
Description:Objectives
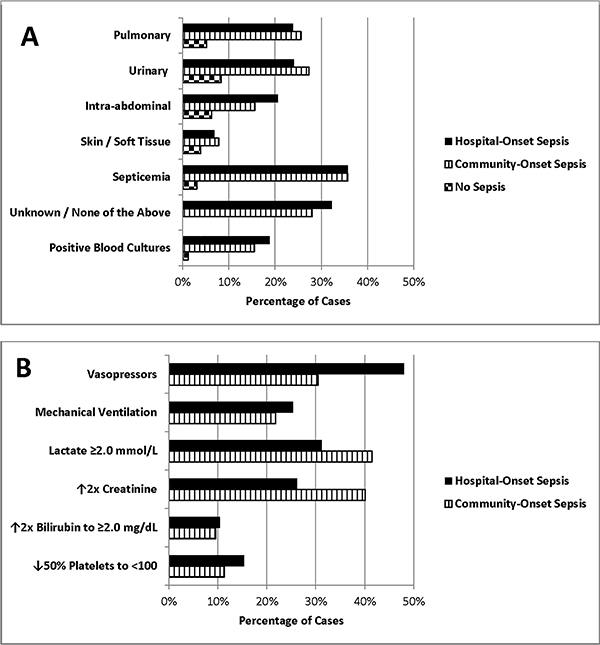
Prior studies have reported that hospital-onset (HO)-sepsis is associated with higher mortality rates than community-onset (CO)-sepsis. Most studies, however, have used inconsistent case-finding methods and applied limited risk-adjustment for potential confounders. We used consistent sepsis criteria and detailed electronic clinical data to elucidate the epidemiology and mortality associated with HO-sepsis.
Design
Retrospective cohort study
Setting
136 U.S. hospitals in the Cerner HealthFacts dataset
Patients
Adults hospitalized in 2009–2015
Interventions
None
Measurements and Main Results
We identified sepsis using CDC Adult Sepsis Event criteria and estimated the risk of in-hospital death for HO-sepsis versus CO-sepsis using logistic regression models. In patients admitted without CO-sepsis, we estimated risk of death associated with HO-sepsis using Cox regression models with sepsis as a time-varying covariate. Models were adjusted for baseline characteristics and severity-of-illness. Among 2.2 million hospitalizations, there were 95,154 sepsis cases: 83,620 (87.9%) CO-sepsis and 11,534 (12.1%) HO-sepsis (0.5% of hospitalized cohort). Compared to CO-sepsis, HO-sepsis patients were younger (median 66 vs 68 years) but had more comorbidities (median Elixhauser score 14 vs 11), higher Sequential Organ Failure Assessment scores (median 4 vs 3), higher ICU admission rates (61% vs 44%), longer hospital length-of-stay (median 19 vs 8 days), and higher in-hospital mortality (33% vs 17%) (p<0.001 for all comparisons). On multivariate analysis, HO-sepsis was associated with higher mortality versus CO-sepsis (odds ratio 2.1, 95% CI 2.0–2.2) and patients admitted without sepsis (hazard ratio 3.0, 95% CI 2.9–3.2).
Conclusions
HO-sepsis complicated 1 in 200 hospitalizations and accounted for 1 in 8 sepsis cases, with 1 in 3 patients dying in-hospital. HO-sepsis preferentially afflicted ill patients but even after risk-adjustment they were twice as likely to die as CO-sepsis patients; in patients admitted without sepsis, HO-sepsis tripled the risk of death. HO-sepsis is an important target for surveillance, prevention, and quality improvement initiatives.
-
Subjects:
-
Source:Crit Care Med. 47(9):1169-1176
-
Pubmed ID:31135503
-
Pubmed Central ID:PMC6697188
-
Document Type:
-
Funding:
-
Place as Subject:
-
Volume:47
-
Issue:9
-
Collection(s):
-
Main Document Checksum:urn:sha256:71d5d38190a94d47e211b5463358384b93b19270bf1bcfcfac0d3e626e81fda5
-
Download URL:
-
File Type:
 [PDF
- 389.21 KB
]
[PDF
- 389.21 KB
]

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access