Neuraminidase inhibitors, superinfection and corticosteroids affect survival of influenza patients
Supporting Files

-
January 08 2015
-
File Language:
English
Details
-
Alternative Title:Eur Respir J
-
Personal Author:
-
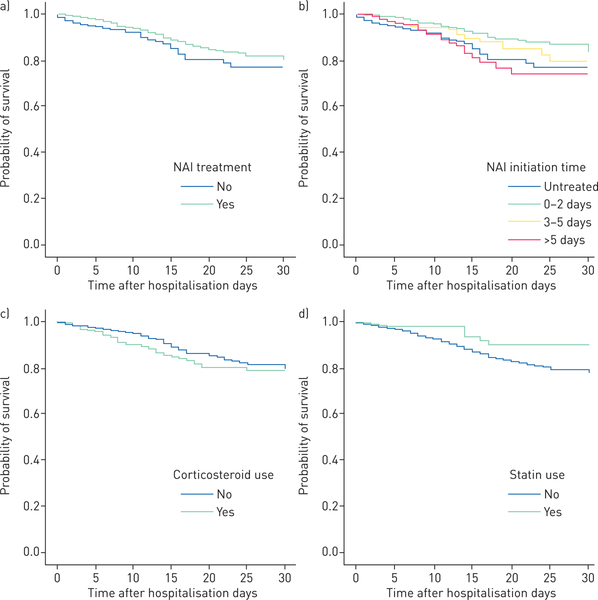
Description:We aimed to study factors influencing outcomes of adults hospitalised for seasonal and pandemic influenza. Individual-patient data from three Asian cohorts (Hong Kong, Singapore and Beijing; N=2649) were analysed. Adults hospitalised for laboratory-confirmed influenza (prospectively diagnosed) during 2008-2011 were studied. The primary outcome measure was 30-day survival. Multivariate Cox regression models (time-fixed and time-dependent) were used. Patients had high morbidity (respiratory/nonrespiratory complications in 68.4%, respiratory failure in 48.6%, pneumonia in 40.8% and bacterial superinfections in 10.8%) and mortality (5.9% at 30 days and 6.9% at 60 days). 75.2% received neuraminidase inhibitors (NAI) (73.8% received oseltamivir and 1.4% received peramivir/zanamivir; 44.5% of patients received NAI ≤2 days and 65.5% ≤5 days after onset of illness); 23.1% received systemic corticosteroids. There were fewer deaths among NAI-treated patients (5.3% versus 7.6%; p=0.032). NAI treatment was independently associated with survival (adjusted hazard ratio (HR) 0.28, 95% CI 0.19-0.43), adjusted for treatment-propensity score and patient characteristics. Superinfections increased (adjusted HR 2.18, 95% CI 1.52-3.11) and chronic statin use decreased (adjusted HR 0.44, 95% CI 0.23-0.84) death risks. Best survival was shown when treatment started within ≤2 days (adjusted HR 0.20, 95% CI 0.12-0.32), but there was benefit with treatment within 3-5 days (adjusted HR 0.35, 95% CI 0.21-0.58). Time-dependent analysis showed consistent results of NAI treatment (adjusted HR 0.39, 95% CI 0.27-0.57). Corticosteroids increased superinfection (9.7% versus 2.7%) and deaths when controlled for indications (adjusted HR 1.73, 95% CI 1.14-2.62). Early NAI treatment was associated with shorter length of stay in a subanalysis. NAI treatment may improve survival of hospitalised influenza patients; benefit is greatest from, but not limited to, treatment started within 2 days of illness. Superinfections and corticosteroids increase mortality. Antiviral and non-antiviral management strategies should be considered.
-
Subjects:
-
Source:Eur Respir J. 45(6):1642-1652
-
Pubmed ID:25573405
-
Pubmed Central ID:PMC6669032
-
Document Type:
-
Funding:
-
Volume:45
-
Issue:6
-
Collection(s):
-
Main Document Checksum:urn:sha256:7c5cf56500bfd8522a56398c235eb703df77713083c7c037742404da7beacc1f
-
Download URL:
-
File Type:
 [PDF
- 482.88 KB
]
[PDF
- 482.88 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access