Analysis of False-Negative Human Immunodeficiency Virus Rapid Tests Performed on Oral Fluid in 3 International Clinical Research Studies
Supporting Files

-
Jun 15 2017
-
File Language:
English
Details
-
Journal Article:Clin Infect Dis
-
Personal Author:
-
Corporate Authors:
-
Description:Background
The OraQuick Advance Rapid HIV-1/2 Test is a point-of-care test capable of detecting human immunodeficiency virus (HIV)-specific antibodies in blood and oral fluid. To understand test performance and factors contributing to false-negative results in longitudinal studies, we examined results of participants enrolled in the Botswana TDF/FTC Oral HIV Prophylaxis Trial, the Bangkok Tenofovir Study, and the Bangkok MSM Cohort Study, 3 separate clinical studies of high-risk, HIV-negative persons conducted in Botswana and Thailand.
Methods
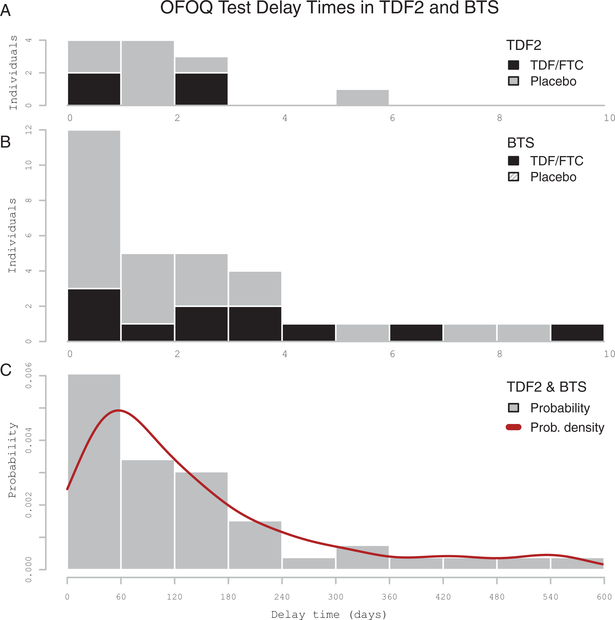
In a retrospective observational analysis, we compared oral fluid OraQuick (OFOQ) results among participants becoming HIV infected to results obtained retrospectively using enzyme immunoassay and nucleic acid amplification tests on stored specimens. We categorized negative OFOQ results as true-negative or false-negative relative to nucleic acid amplification test and/ or enzyme immunoassay, and determined the delay in OFOQ conversion relative to the estimated time of infection. We used log-binomial regression and generalized estimating equations to examine the association between false-negative results and participant, clinical, and testing-site factors.
Results
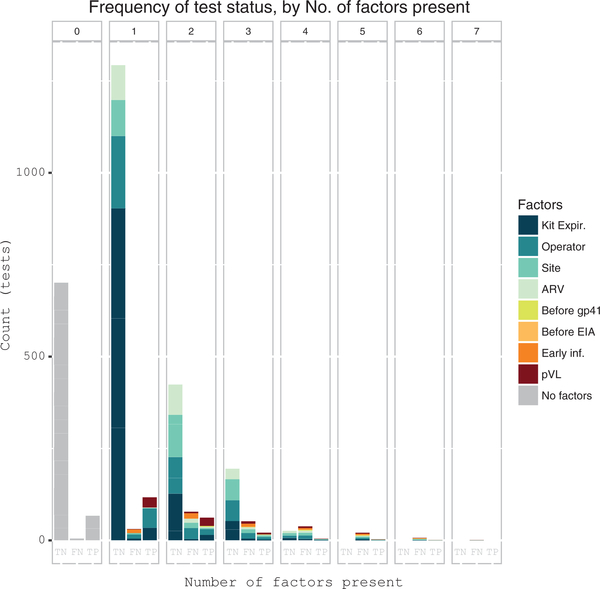
Two-hundred thirty-three false-negative OFOQ results occurred in 80 of 287 seroconverting individuals. Estimated OFOQ conversion delay ranged from 14.5 to 547.5 (median, 98.5) days. Delayed OFOQ conversion was associated with clinical site and test operator (P < .05), preexposure prophylaxis (P = .01), low plasma viral load (P < .02), and time to kit expiration (P < .01). Participant age, sex, and HIV subtype were not associated with false-negative results. Long OFOQ conversion delay time was associated with antiretroviral exposure and low plasma viral load.
Conclusions
Failure of OFOQ to detect HIV-1 infection was frequent and multifactorial in origin. In longitudinal trials, negative oral fluid results should be confirmed via testing of blood samples.
-
Subjects:
-
Source:Clin Infect Dis. 64(12):1663-1669
-
DOI:
-
Pubmed ID:28369309
-
Pubmed Central ID:PMC6502462
-
Document Type:
-
Funding:
-
Genre:
-
Volume:64
-
Issue:12
-
Collection(s):
-
Main Document Checksum:urn:sha-512:5ce63fca2c9324c980f4969203ce88cb972c1f4e4c3b73a03820880f926efd1de5b338f71454b6f7daf8c18e1bb7ea1e5f010d275e02d5d657c2a317b147a345
-
Download URL:
-
File Type:
 [PDF
- 276.02 KB
]
[PDF
- 276.02 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access