Universal versus conditional day 3 follow-up for children with non-severe unclassified fever at the community level in Ethiopia: A cluster-randomised non-inferiority trial
Supporting Files
Public Domain

-
Apr 17 2018
-
File Language:
English
Details
-
Alternative Title:PLoS Med
-
Personal Author:
-
Description:Background
With declining malaria prevalence and improved use of malaria diagnostic tests, an increasing proportion of children seen by community health workers (CHWs) have unclassified fever. Current community management guidelines by WHO advise that children seen with non-severe unclassified fever (on day 1) should return to CHWs on day 3 for reassessment. We compared the safety of conditional follow-up reassessment only in cases where symptoms do not resolve with universal follow-up on day 3.
Methods and findings
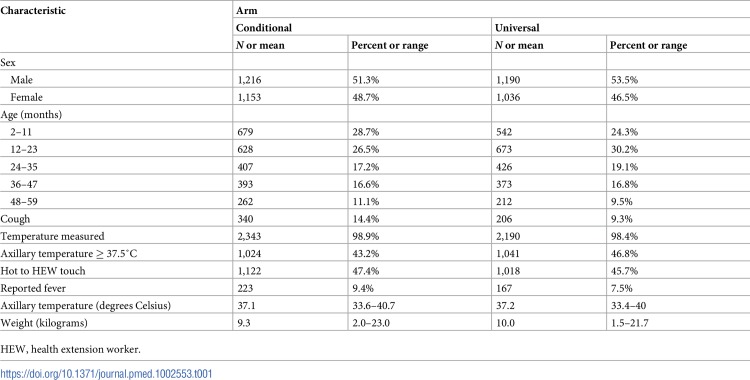
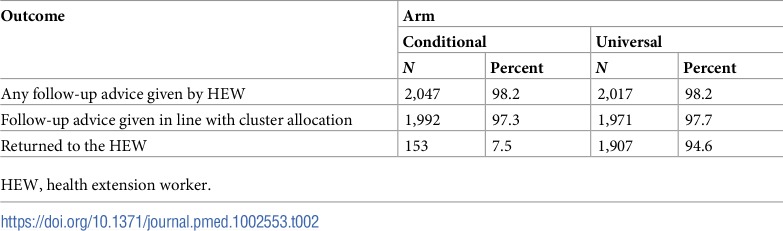
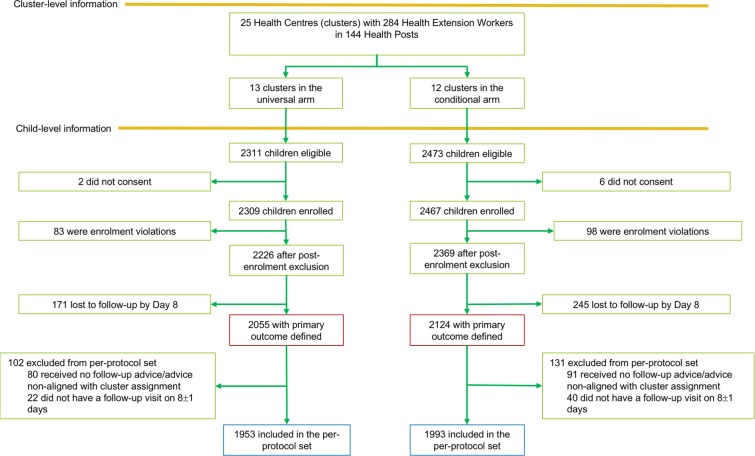
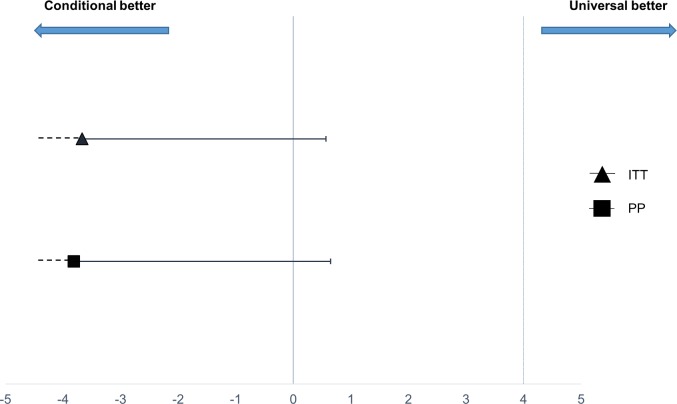
We undertook a 2-arm cluster-randomised controlled non-inferiority trial among children aged 2–59 months presenting with fever and without malaria, pneumonia, diarrhoea, or danger signs to 284 CHWs affiliated with 25 health centres (clusters) in Southern Nations, Nationalities, and Peoples’ Region, Ethiopia. The primary outcome was treatment failure (persistent fever, development of danger signs, hospital admission, death, malaria, pneumonia, or diarrhoea) at 1 week (day 8) of follow-up. Non-inferiority was defined as a 4% or smaller difference in the proportion of treatment failures with conditional follow-up compared to universal follow-up. Secondary outcomes included the percentage of children brought for reassessment, antimicrobial prescription, and severe adverse events (hospitalisations and deaths) after 4 weeks (day 29). From December 1, 2015, to November 30, 2016, we enrolled 4,595 children, of whom 3,946 (1,953 universal follow-up arm; 1,993 conditional follow-up arm) adhered to the CHW’s follow-up advice and also completed a day 8 study visit within ±1 days. Overall, 2.7% had treatment failure on day 8: 0.8% (16/1,993) in the conditional follow-up arm and 4.6% (90/1,953) in the universal follow-up arm (risk difference of treatment failure −3.81%, 95% CI −∞, 0.65%), meeting the prespecified criterion for non-inferiority. There were no deaths recorded by day 29. In the universal follow-up arm, 94.6% of caregivers reported returning for reassessment on day 3, in contrast to 7.5% in the conditional follow-up arm (risk ratio 22.0, 95% CI 17.9, 27.2, p < 0.001). Few children sought care from another provider after their initial visit to the CHW: 3.0% (59/1,993) in the conditional follow-up arm and 1.1% (22/1,953) in the universal follow-up arm, on average 3.2 and 3.4 days later, respectively, with no significant difference between arms (risk difference 1.79%, 95% CI −1.23%, 4.82%, p = 0.244). The mean travel time to another provider was 2.2 hours (95% CI 0.01, 5.3) in the conditional follow-up arm and 2.6 hours (95% CI 0.02, 4.5) in the universal follow-up arm (p = 0.82); the mean cost for seeking care after visiting the CHW was 26.5 birr (95% CI 7.8, 45.2) and 22.8 birr (95% CI 15.6, 30.0), respectively (p = 0.69). Though this study was an important step to evaluate the safety of conditional follow-up, the high adherence seen may have resulted from knowledge of the 1-week follow-up visit and may therefore not transfer to routine practice; hence, in an implementation setting it is crucial that CHWs are well trained in counselling skills to advise caregivers on when to come back for follow-up.
Conclusions
Conditional follow-up of children with non-severe unclassified fever in a low malaria endemic setting in Ethiopia was non-inferior to universal follow-up through day 8. Allowing CHWs to advise caregivers to bring children back only in case of continued symptoms might be a more efficient use of resources in similar settings.
Trial registration
www.clinicaltrials.gov, identifier NCT02926625
Why was this study done?
What did the researchers do and find?
What do these findings mean?
-
Subjects:
-
Source:PLoS Med. 15(4).
-
Pubmed ID:29664899
-
Pubmed Central ID:PMC5903591
-
Document Type:
-
Place as Subject:
-
Volume:15
-
Issue:4
-
Collection(s):
-
Main Document Checksum:urn:sha256:15a78fe8e50642a696aa220d279c3bce3f585ad3c2a51534e9ade75d91e34aed
-
Download URL:
-
File Type:
 [PDF
- 1.50 MB
]
[PDF
- 1.50 MB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access