A METRIC OF OUR OWN: FAILURE TO RESCUE AFTER TRAUMA
Supporting Files

-
Oct 2017
-
File Language:
English
Details
-
Alternative Title:J Trauma Acute Care Surg
-
Personal Author:
-
Description:Background
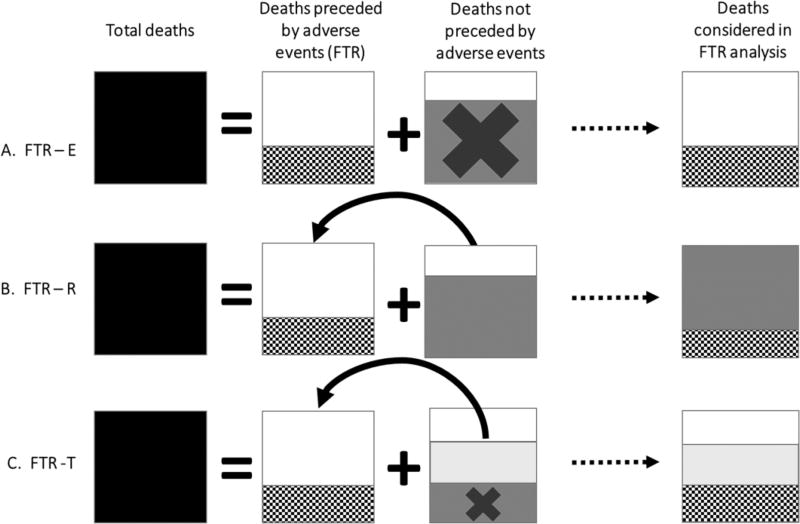
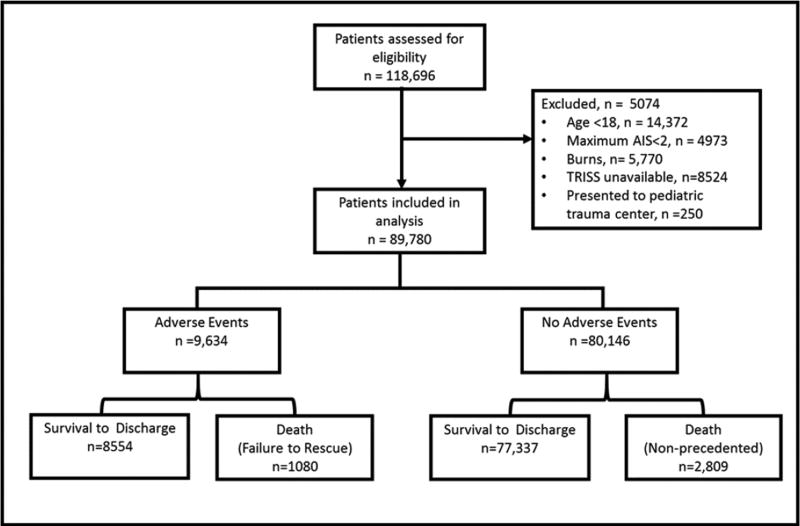
Failure to rescue (FTR) is defined as death after an adverse event. The original metric was derived in elective surgical populations and reclassifies deaths not preceded by recorded adverse events as FTR cases under the assumption these deaths resulted from missed adverse events. This approach lacks face validity in trauma because patients often die without adverse events as a direct result of injury. Another common approach simply excludes deaths without recorded adverse events, but this approach reduces the reliability of the FTR metric. We hypothesized that a hybrid metric excluding expected deaths but otherwise including patients without recorded adverse events in FTR analysis would improve face validity and reliability relative to existing methods.
Methods
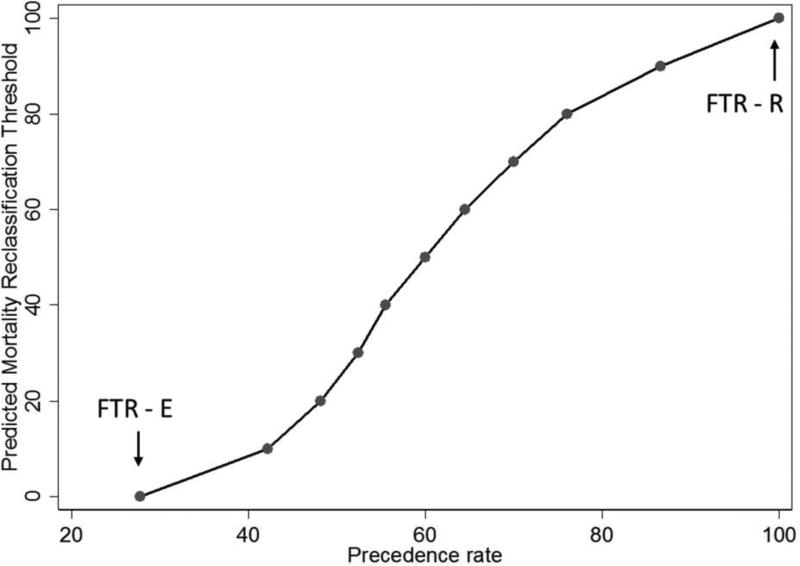
Using 3 years of single-state adult trauma registry data from 30 trauma centers, we constructed 3 FTR metrics: 1.) Excluding deaths not preceded by adverse events (FTR-E), 2.) Reclassifying deaths not preceded by adverse events (FTR-R), and 2.) Including deaths not preceded by adverse events in FTR analysis except those with predicted mortality >50% (FTR-T). Mortality, adverse event, and FTR rates were calculated under each method, and reliability was tested using Spearman’s correlation for split-sample center rankings.
Results
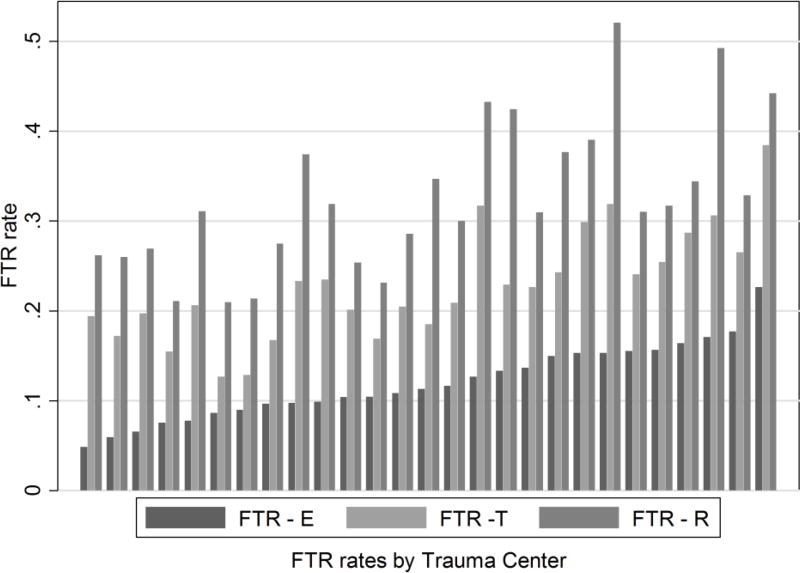
A total of 89,780 patients were included (median age 57 (IQR 26–73), 85% Caucasian, 59% male, 92% blunt, median ISS 9 (IQR5–14)). FTR rates varied by metric (FTR-E: 11.2%; FTR-R 31.2%; FTR-T 21.4%)), as did the proportion of deaths preceded by adverse events (FTR-E 28%; FTR-R: 100%; FTR-T: 60%). Spit-sample reliability was higher FTR-T than FTR-E (rho=0.59 vs) (rho=0.27, p<0.001).
Conclusions
A trauma-specific FTR metric increases face validity and reliability relative to other FTR methods which may be employed in trauma populations. Future trauma outcomes studies examining FTR rates should use a metric designed for this cohort.
Level of Evidence
Level III
-
Subjects:
-
Source:J Trauma Acute Care Surg. 83(4):698-704.
-
Pubmed ID:28538625
-
Pubmed Central ID:PMC5608646
-
Document Type:
-
Funding:
-
Place as Subject:
-
Volume:83
-
Issue:4
-
Collection(s):
-
Main Document Checksum:urn:sha256:f1e7a4192c11b4ec5ca18c3c057e65b4febaade4e7df3254d0ec764d4fbbe4b6
-
Download URL:
-
File Type:
 [PDF
- 1.67 MB
]
[PDF
- 1.67 MB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access