The optimal age for screening adolescents and young adults without identified risk factors for HIV
Supporting Files

-
1 2018
-
File Language:
English
Details
-
Alternative Title:J Adolesc Health
-
Personal Author:
-
Description:Purpose
To assess the optimal age at which a one-time HIV screen should begin for adolescents and young adults (AYA) in the United States without identified HIV risk factors, incorporating clinical impact, costs, and cost-effectiveness.
Methods
We simulated HIV-uninfected 12-year-olds in the US without identified risk factors who faced age-specific risks of HIV infection (0.6–71.3/100,000PY). We modeled a one-time screen ($36) at age 15, 18, 21, 25, or 30, each in addition to current US screening practices (30% screened by age 24). Outcomes included retention in care, virologic suppression, life expectancy, lifetime costs and incremental cost-effectiveness ratios in $/year-of-life saved (YLS) from the healthcare system perspective. In sensitivity analyses, we varied HIV incidence, screening and linkage rates, and costs.
Results
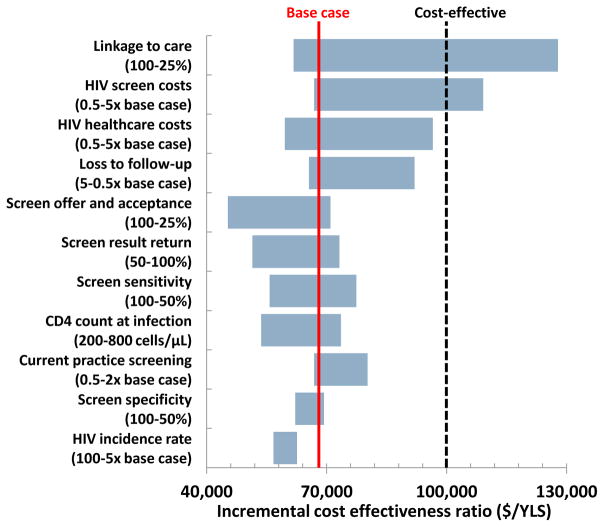
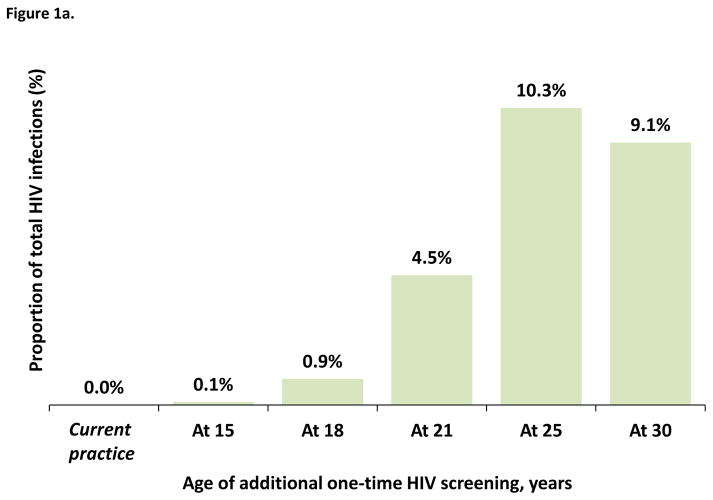
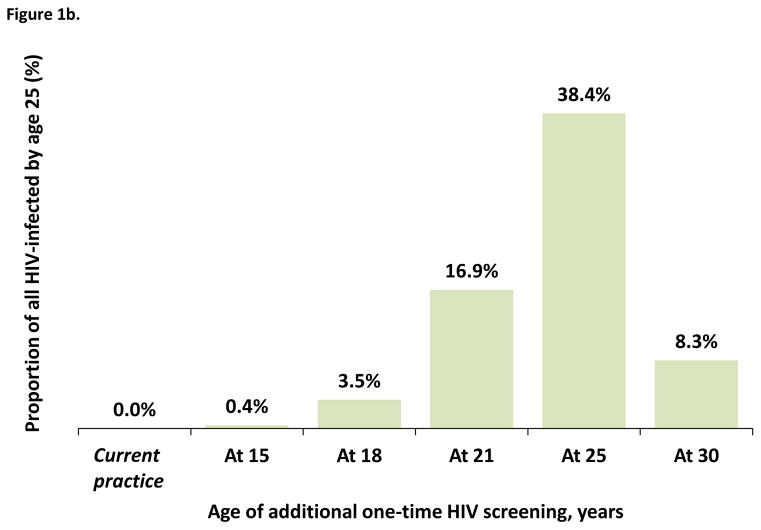
All one-time screens detected a small proportion of lifetime infections (0.1–10.3%). Compared to current US screening practices, a screen at age 25 led to the most favorable care continuum outcomes at age 25: proportion diagnosed (77% vs. 51%), linked to care (71% vs. 51%), retained in care (68% vs. 44%) and virologically suppressed (49% vs. 32%). Compared to the next most effective screen, a screen at age 25 provided the greatest clinical benefit, and was cost-effective ($96,000/YLS) by US standards (<$100,000/YLS).
Conclusions
For US AYA without identified risk factors, a one-time routine HIV screen at age 25, after the peak of incidence, would optimize clinical outcomes and be cost-effective compared to current US screening practices. Focusing screening on AYA ages 18 or younger is a less efficient use of a one-time screen among AYA than screening at a later age.
-
Subjects:
-
Keywords:
-
Source:J Adolesc Health. 62(1):22-28
-
Pubmed ID:29273141
-
Pubmed Central ID:PMC5745059
-
Document Type:
-
Funding:
-
Volume:62
-
Issue:1
-
Collection(s):
-
Main Document Checksum:urn:sha-512:9ceb41a4bfa640b2da97a3b6bd7b5475729d88d574bb094a19218c5fbbd6166da106c1d1416fc5d5e284fb0db88d9a51feb4e7e7022dedfa90ed11b11833982e
-
Download URL:
-
File Type:
 [PDF
- 483.93 KB
]
[PDF
- 483.93 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access