Program
Supporting Files
Public Domain

-
Apr 04 2011
-
File Language:
English
Details
-
Alternative Title:PLoS One
-
Personal Author:
-
Description:Background
In Mozambique during 2004–2007 numbers of adult patients (≥15 years old) enrolled on antiretroviral therapy (ART) increased about 16-fold, from <5,000 to 79,500. All ART patients were eligible for co-trimoxazole. ART program outcomes, and determinants of outcomes, have not yet been reported.
Methodology/Principal Findings
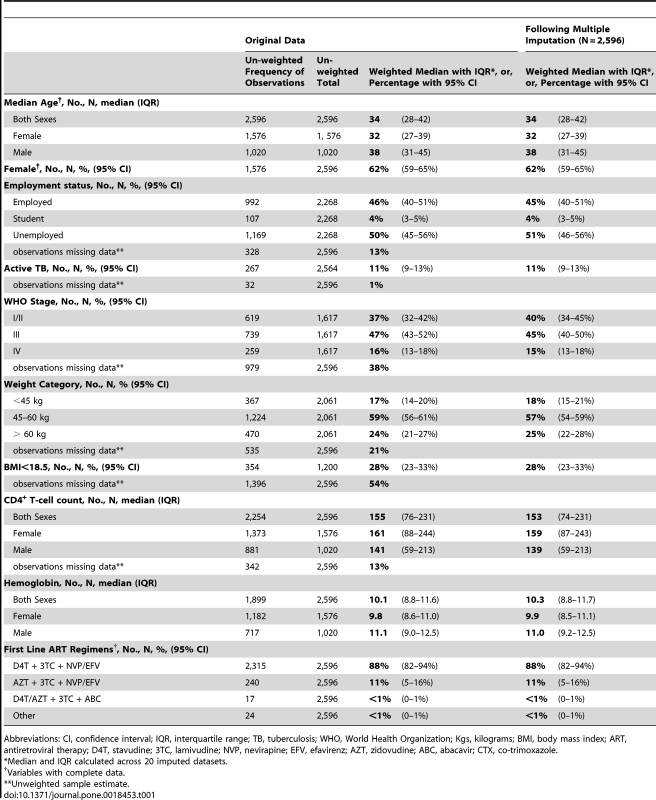
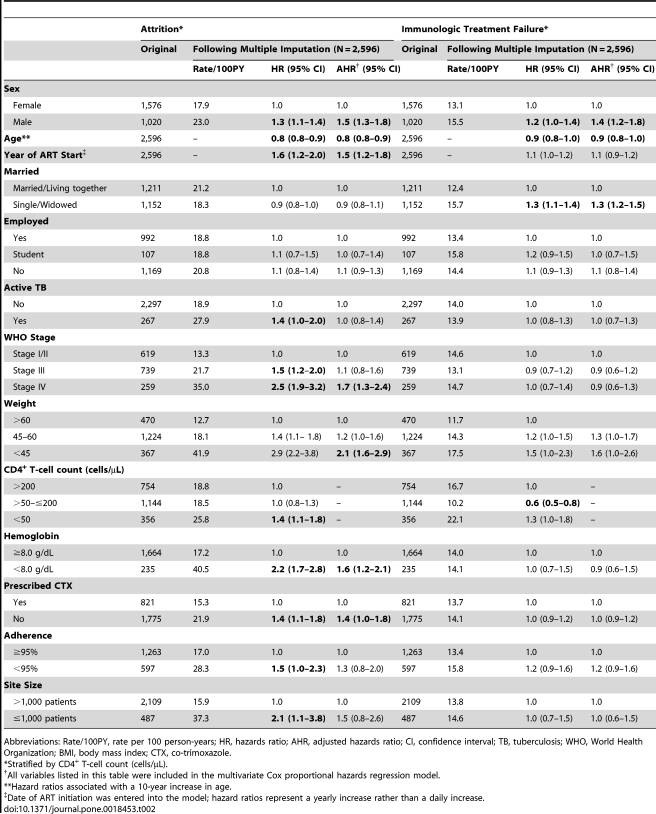
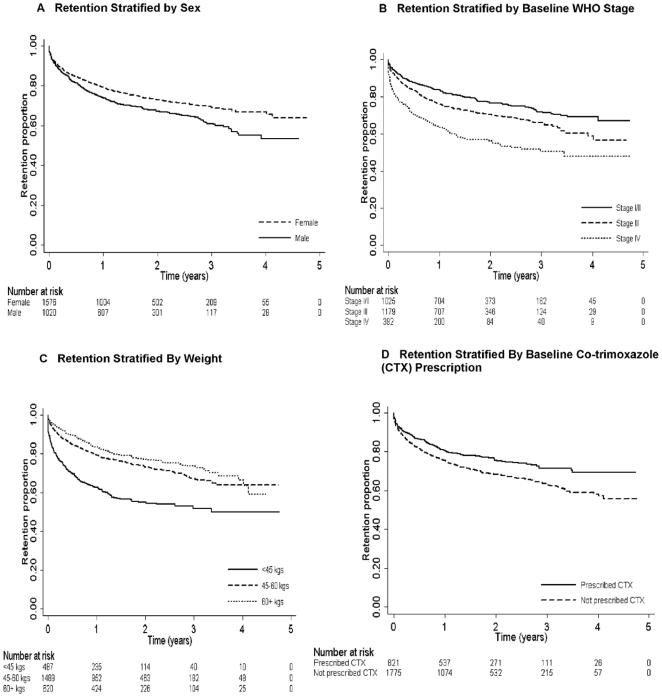
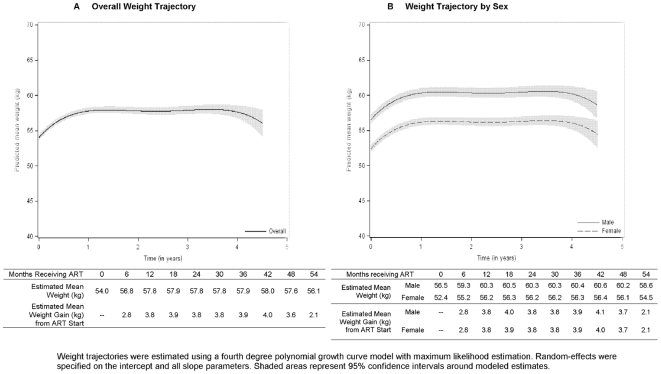
In a retrospective cohort study, we investigated rates of mortality, attrition (death, loss to follow-up, or treatment cessation), immunologic treatment failure, and regimen-switch, as well as determinants of selected outcomes, among a nationally representative sample of 2,596 adults initiating ART during 2004–2007. At ART initiation, median age of patients was 34 and 62% were female. Malnutrition and advanced disease were common; 18% of patients weighed <45 kilograms, and 15% were WHO stage IV. Median baseline CD4+ T-cell count was 153/µL and was lower for males than females (139/µL vs. 159/µL, p<0.01). Stavudine, lamivudine, and nevirapine or efavirenz were prescribed to 88% of patients; only 31% were prescribed co-trimoxazole. Mortality and attrition rates were 3.4 deaths and 19.8 attritions per 100 patient-years overall, and 12.9 deaths and 57.2 attritions per 100 patient-years in the first 90 days. Predictors of attrition included male sex [adjusted hazard ratio (AHR) 1.5; 95% confidence interval (CI), 1.3–1.8], weight <45 kg (AHR 2.1; 95% CI, 1.6–2.9, reference group >60 kg), WHO stage IV (AHR 1.7; 95% CI, 1.3–2.4, reference group WHO stage I/II), lack of co-trimoxazole prescription (AHR 1.4; 95% CI, 1.0–1.8), and later calendar year of ART initiation (AHR 1.5; 95% CI, 1.2–1.8). Rates of immunologic treatment failure and regimen-switch were 14.0 and 0.6 events per 100-patient years, respectively.
Conclusions
ART initiation at earlier disease stages and scale-up of co-trimoxazole among ART patients could improve outcomes. Research to determine reasons for low regimen-switch rates and increasing rates of attrition during program expansion is needed.
-
Subjects:
-
Source:PLoS One. 6(4).
-
Pubmed ID:21483703
-
Pubmed Central ID:PMC3070740
-
Document Type:
-
Place as Subject:
-
Volume:6
-
Issue:4
-
Collection(s):
-
Main Document Checksum:urn:sha-512:8c27f453b5cd19ebf6b9013a6299725e8b38d5f0f9b4b3a5d61d4e2e9d08efb8c600e78beae437db7baae4d9b481d398a22953bddec6c20f358af220f2564819
-
Download URL:
-
File Type:
 [PDF
- 465.92 KB
]
[PDF
- 465.92 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access