Cost-Effectiveness of Antiretroviral Therapy and Isoniazid Prophylaxis to Reduce Tuberculosis and Death in People Living With HIV in Botswana
Supporting Files

-
Nov 01 2015
-
File Language:
English
Details
-
Alternative Title:J Acquir Immune Defic Syndr
-
Personal Author:
-
Description:Objective
In Botswana, a 36-month course of isoniazid treatment of latent tuberculosis (TB) infection [isoniazid preventive therapy (IPT)] was superior to 6-month IPT in reducing TB and death in persons living with HIV (PLHIV), having positive tuberculin skin tests (TSTs) but not in those with negative TST. We examined the cost-effectiveness of IPT in Botswana, where antiretroviral therapy (ART) is widely available.
Design
Using a decision-analytic model, we determined the incremental cost-effectiveness of strategies for reducing TB and death in 10,000 PLHIV over 36 months.
Methods
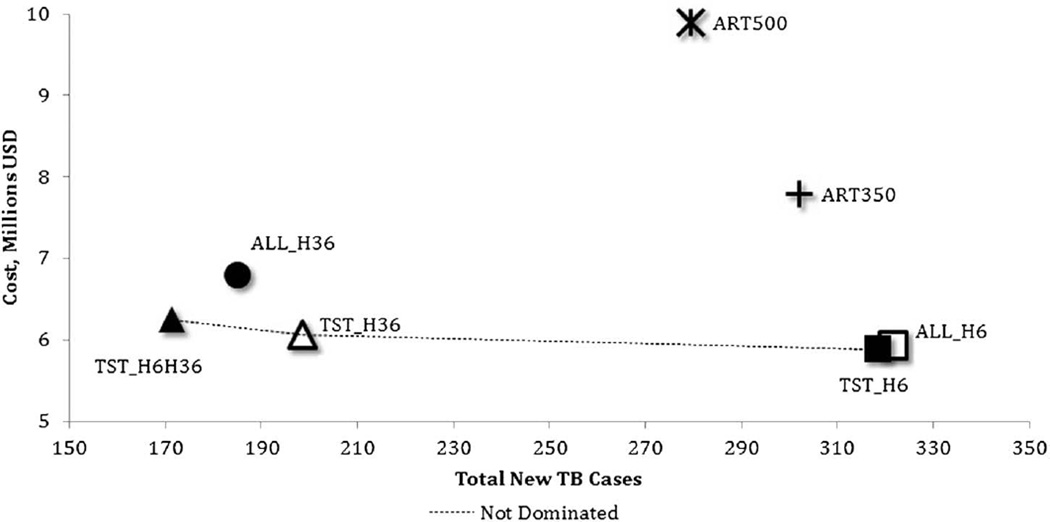
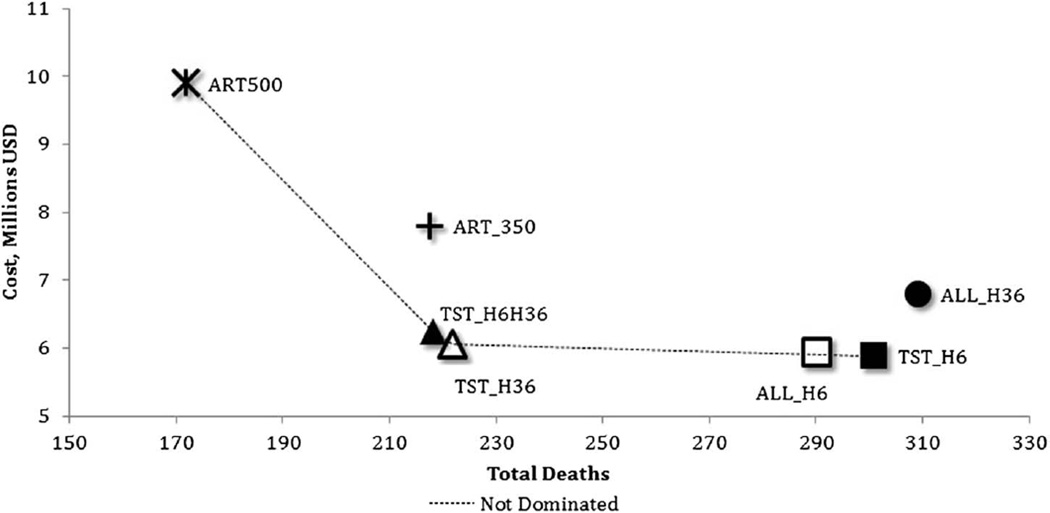
IPT for 6 months and provision of ART if CD4+ lymphocyte count <250 cells per microliter (2011 Botswana policy) was compared with 6 alternative strategies that varied the use of IPT, TST, and ART for CD4+ count thresholds, including CD4+ <350 and <500 cells per microliter.
Results
Botswana policy, 2011 was dominated by most other strategies. IPT of 36 months for TST-positive PLHIV with ART for CD4+ <250 cells per microliter resulted in 120 fewer TB cases for an additional cost of $1612 per case averted and resulted in 80 fewer deaths for an additional $2418 per death averted compared with provision of 6-month IPT to TST-positive PLHIV who received ART for CD4+ <250 cells per microliter, the next most effective strategy. Alternative strategies offered lower incremental effectiveness at higher cost. These findings remained consistent in sensitivity analyses.
Conclusions
A strategy of treating PLHIV who have positive TST with 36-month IPT is more cost effective for reducing both TB and death compared with providing IPT without a TST, providing only 6-month IPT, or expanding ART eligibility without IPT.
-
Subjects:
-
Source:J Acquir Immune Defic Syndr. 70(3):e84-e93
-
Pubmed ID:26258564
-
Pubmed Central ID:PMC5131632
-
Document Type:
-
Funding:
-
Volume:70
-
Issue:3
-
Collection(s):
-
Main Document Checksum:urn:sha256:ef340e0a47e8a3e24ea1c1482f2e1878ed6ac2a5ee2a01837126b8616cbc9e96
-
Download URL:
-
File Type:
 [PDF
- 780.97 KB
]
[PDF
- 780.97 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access