Retention of HIV-infected children on antiretroviral treatment in HIV care and treatment programs in Kenya, Mozambique, Rwanda and Tanzania
Supporting Files

-
03/01/2013
-
File Language:
English
Details
-
Alternative Title:J Acquir Immune Defic Syndr
-
Personal Author:
-
Corporate Authors:
-
Description:Background
Retention of children in HIV care is essential for prevention of disease progression and mortality.
Methods
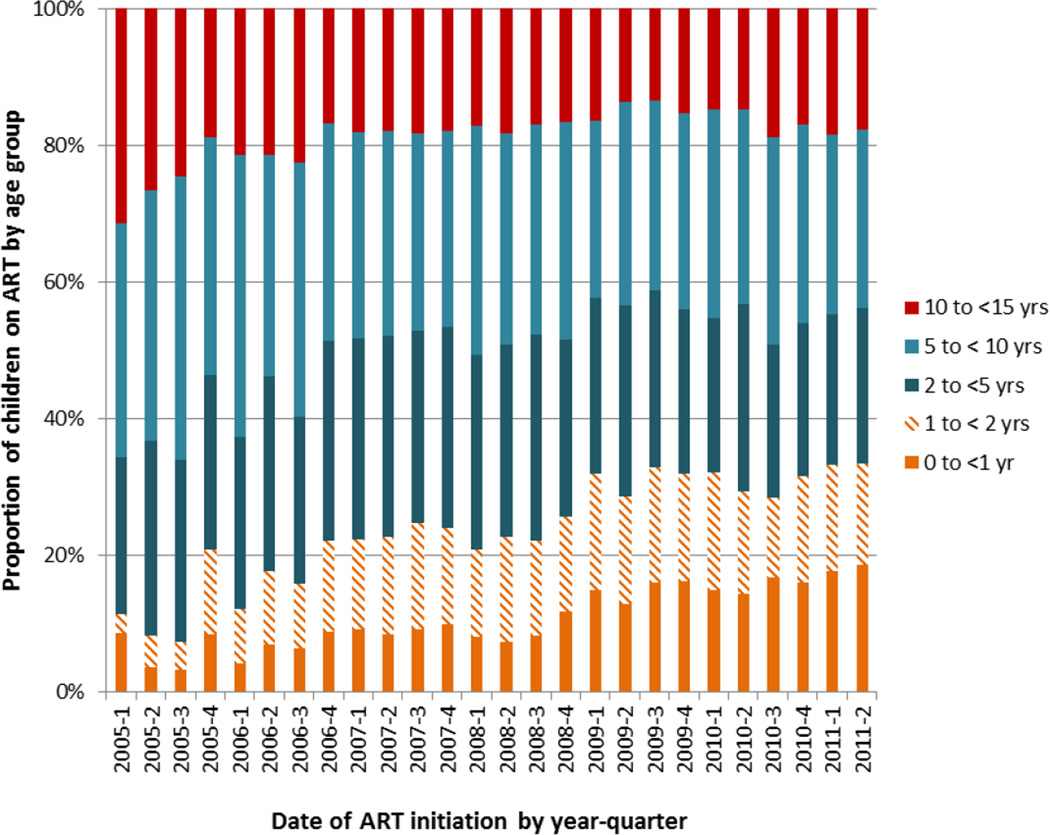
Retrospective cohort of children (0 to <15 years) initiating antiretroviral treatment (ART) at health facilities in Kenya, Mozambique, Rwanda and Tanzania, January 2005–June 2011. Retention was defined as the proportion of children known to be alive and attending care at their initiation facility; lost to follow-up (LTF) was defined as no clinic visit for > 6 months. Cumulative incidence of ascertained survival and retention after ART initiation was estimated through 24 months using Kaplan-Meier methods. Factors associated with LTF and death were assessed using Cox proportional hazard modeling.
Results
17,712 children initiated ART at 192 facilities: median age was 4.6 years (IQR: 1.9–8.3), median CD4 was 15% (IQR: 10–20) for children < 5 years and 265 cells/uL (IQR: 111–461) for children ≥ 5 years. At 12 and 24 months, 80% and 72% of children were retained with 16% and 22% LTF and 5% and 7% known deaths respectively. Retention ranged from 71–95% and 62–93% at 12 and 24 months across countries, and was lowest for children < 1 year (51% at 24 months). LTF and death were highest in children < 1 year of age and children with advanced disease.
Conclusion
Retention was lowest in young children and differed across country programs. Young children and those with advanced disease are at highest risk for LTF and death. Further evaluation of patient- and program-level factors is needed to improve health outcomes.
-
Keywords:
-
Source:J Acquir Immune Defic Syndr. 62(3):e70-e81
-
Pubmed ID:23111575
-
Pubmed Central ID:PMC5094048
-
Document Type:
-
Funding:
-
Place as Subject:
-
Volume:62
-
Issue:3
-
Collection(s):
-
Main Document Checksum:urn:sha256:06a067aff4e9a85e852e4525589bb7642f68261cd7bd5e85595129cf616dfb9a
-
Download URL:
-
File Type:
 [PDF
- 837.00 KB
]
[PDF
- 837.00 KB
]
Supporting Files

File Language:
English

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access