Cost-Effectiveness of Pooled Nucleic Acid Amplification Testing for Acute HIV Infection after Third-Generation HIV Antibody Screening and Rapid Testing in the United States: A Comparison of Three Public Health Settings
Supporting Files
Public Domain

-
Sep 28 2010
-
File Language:
English
Details
-
Alternative Title:PLoS Med
-
Personal Author:
-
Description:Background
Detection of acute HIV infection (AHI) with pooled nucleic acid amplification testing (NAAT) following HIV testing is feasible. However, cost-effectiveness analyses to guide policy around AHI screening are lacking; particularly after more sensitive third-generation antibody screening and rapid testing.
Methods and Findings
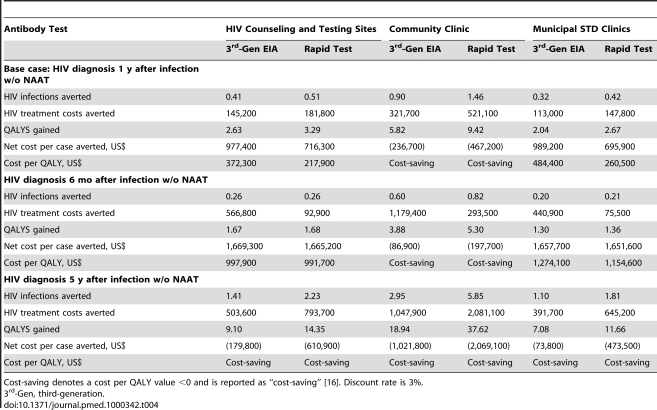
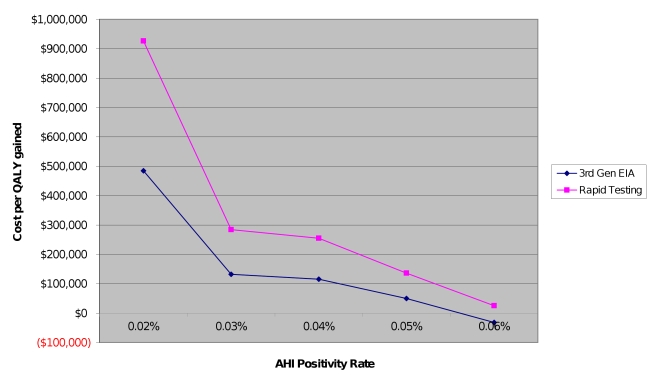
We conducted a cost-effectiveness analysis of pooled NAAT screening that assessed the prevention benefits of identification and notification of persons with AHI and cases averted compared with repeat antibody testing at different intervals. Effectiveness data were derived from a Centers for Disease Control and Prevention AHI study conducted in three settings: municipal sexually transmitted disease (STD) clinics, a community clinic serving a population of men who have sex with men, and HIV counseling and testing sites. Our analysis included a micro-costing study of NAAT and a mathematical model of HIV transmission. Cost-effectiveness ratios are reported as costs per quality-adjusted life year (QALY) gained in US dollars from the societal perspective. Sensitivity analyses were conducted on key variables, including AHI positivity rates, antibody testing frequency, symptomatic detection of AHI, and costs. Pooled NAAT for AHI screening following annual antibody testing had cost-effectiveness ratios exceeding US$200,000 per QALY gained for the municipal STD clinics and HIV counseling and testing sites and was cost saving for the community clinic. Cost-effectiveness ratios increased substantially if the antibody testing interval decreased to every 6 months and decreased to cost-saving if the testing interval increased to every 5 years. NAAT was cost saving in the community clinic in all situations. Results were particularly sensitive to AHI screening yield.
Conclusions
Pooled NAAT screening for AHI following negative third-generation antibody or rapid tests is not cost-effective at recommended antibody testing intervals for high-risk persons except in very high-incidence settings.
Please see later in the article for the Editors' Summary
Since 1981, acquired immunodeficiency syndrome (AIDS) has killed about 25 million people and about 30 million people are now infected with the human immunodeficiency virus (HIV), which causes AIDS. HIV, which is most often transmitted through unprotected sex with an infected partner or injection drug use, infects and kills immune system cells, leaving infected individuals susceptible to other infectious diseases. The first, often undiagnosed stage of HIV infection—acute HIV infection (AHI)—lasts a few weeks and sometimes involves a flu-like illness. During AHI, the immune system responds to HIV by beginning to make antibodies that recognize the virus but seroconversion—the appearance of detectable amounts of antibody in the blood—takes 6–12 weeks. During the second, symptom-free stage of HIV infection, which can last many years, the virus gradually destroys the immune system so that by the third stage of infection unusual infections (for example, persistent yeast infections) begin to occur. The final stage of infection (AIDS) is characterized by multiple severe infections and by the development of unusual cancers.
Why Was This Study Done?
Antiretroviral drugs control HIV infections but don't cure them. It is very important, therefore, to prevent HIV transmission by avoiding HIV risk behaviors that increase the risk of HIV infection such as having sex without a condom or with many partners. Individuals with AHI in particular need to avoid high-risk behaviors because these people are extremely infectious. However, routine tests for HIV infection that measure antibodies in the blood often give false-negative results in people with AHI because of the time lag between infection and seroconversion. Nucleic acid amplification testing (NAAT), which detects HIV genetic material in the blood, is a more accurate way to diagnose AHI but is expensive. In this study, the researchers investigate whether pooled NAAT screening (specimens are pooled before testing to reduce costs) for AHI in clinic settings after third-generation antibody testing is a cost-effective HIV prevention strategy. That is, does the gain in quality-adjusted life years (QALY, a measure of the quantity and quality of life generated by healthcare interventions) achieved by averting new HIV infections outweigh the costs of pooled NAAT screening?
What Did the Researchers Do and Find?
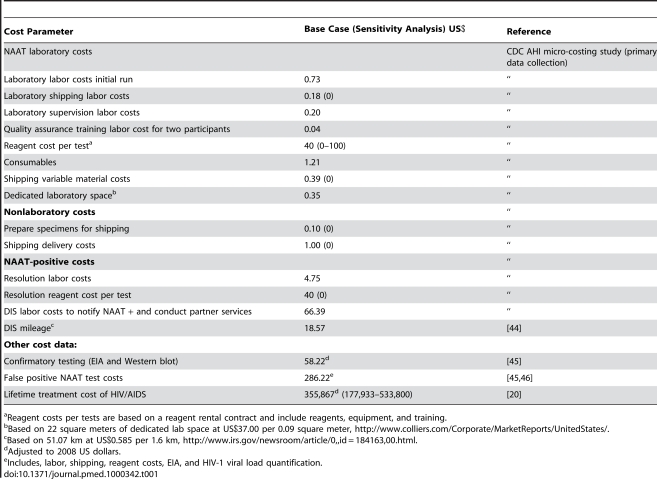
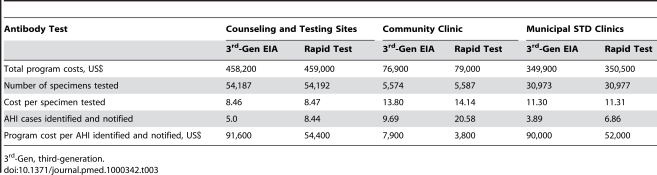
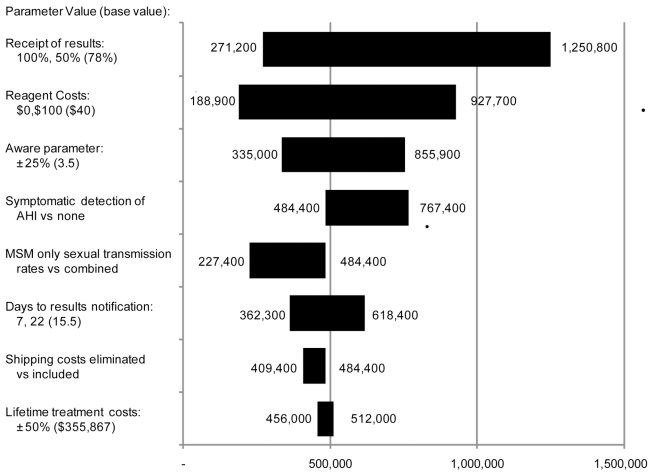
The researchers combined effectiveness data from a US study in which AHI was detected using pooled NAAT in three settings (sexually transmitted disease [STD] clinics, a community clinic serving men who have sex with men [MSM], and HIV counseling/testing sites) with a “micro-costing” study of NAAT and a mathematical model of HIV transmission. They then calculated the costs per QALY gained (the cost-effectiveness ratio) as a result of HIV prevention by identification and notification of people with AHI through pooled NAAT screening compared with repeat antibody testing. Pooled NAAT for AHI screening following annual antibody testing (the recommended testing interval for high-risk individuals), they estimate, would cost US$372,300 and US$484,400 per QALY gained for the counseling/testing sites and STD clinics, respectively, whereas pooled NAAT for AHI screening was cost-saving for the community clinic serving MSM. The cost-effectiveness ratio increased for the counseling/testing sites and STD clinics when the antibody testing interval was decreased to 6 months but remained cost-saving for the community clinic. With an antibody testing interval of 5 years, pooled NAAT was cost-saving in all three settings.
What Do These Findings Mean?
Cost-effectiveness ratios of US$100,000–US$200,000 are considered acceptable in the US. These results suggest therefore, that the cost of pooled NAAT screening for AHI following negative third-generation antibody testing is not acceptable at the recommended testing interval for high-risk individuals except in settings where HIV infection is very common such as clinics serving MSM. The researchers reach a similar conclusion in a separate cost-effectiveness analysis of pooled NAAT screening following a negative rapid HIV test. Although the accuracy of these results depends on numerous assumptions made in the cost-effectiveness analyses (for example, the degree to which awareness of HIV status affects the behavior of people with AHI), sensitivity analyses (investigations of the effect of altering key assumptions) show that these findings are not greatly affected by changes in many of these assumptions. Thus, the researchers conclude, NAAT screening should be reserved for settings that serve populations in which there are very high levels of new HIV infection.
Additional Information
Please access these Web sites via the online version of this summary at http://dx.doi.org/10.1371/journal.pmed.1000342.
-
Subjects:
-
Source:PLoS Med. 7(9).
-
Document Type:
-
Place as Subject:
-
Volume:7
-
Issue:9
-
Collection(s):
-
Main Document Checksum:urn:sha-512:49e6e58bd0542ebc207b57ff52b700a52e797eca609b404376200c3839632031f9faedc7bd79f47cf341cac633a82df1062faf5b3e0554bb0751f90ac0e47c66
-
Download URL:
-
File Type:
 [PDF
- 613.46 KB
]
[PDF
- 613.46 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access