Minority HIV-1 Drug Resistance Mutations Are Present in Antiretroviral Treatment–Naïve Populations and Associate with Reduced Treatment Efficacy
Supporting Files
Public Domain

-
Jul 29 2008
-
File Language:
English
Details
-
Alternative Title:PLoS Med
-
Personal Author:
-
Description:Background
Transmitted HIV-1 drug resistance can compromise initial antiretroviral therapy (ART); therefore, its detection is important for patient management. The absence of drug-associated selection pressure in treatment-naïve persons can cause drug-resistant viruses to decline to levels undetectable by conventional bulk sequencing (minority drug-resistant variants). We used sensitive and simple tests to investigate evidence of transmitted drug resistance in antiretroviral drug-naïve persons and assess the clinical implications of minority drug-resistant variants.
Methods and Findings
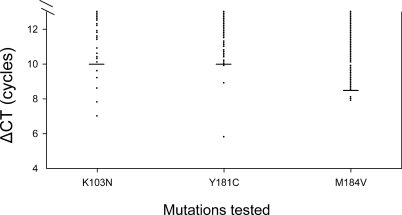
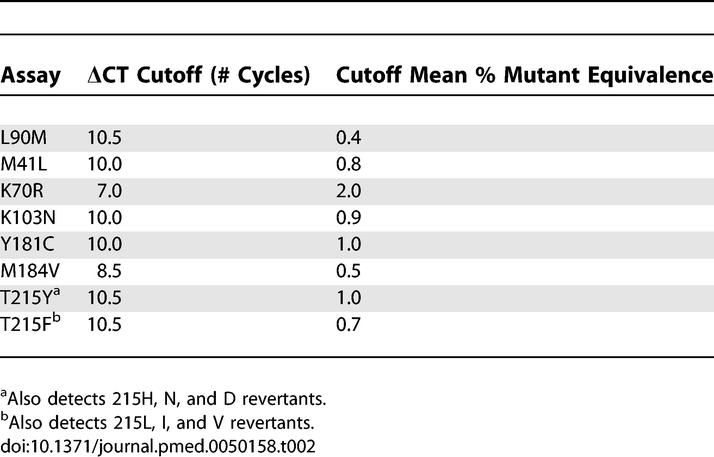
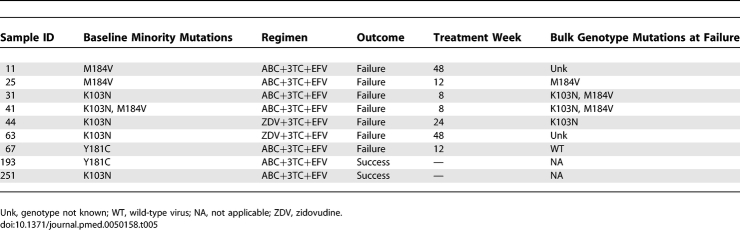
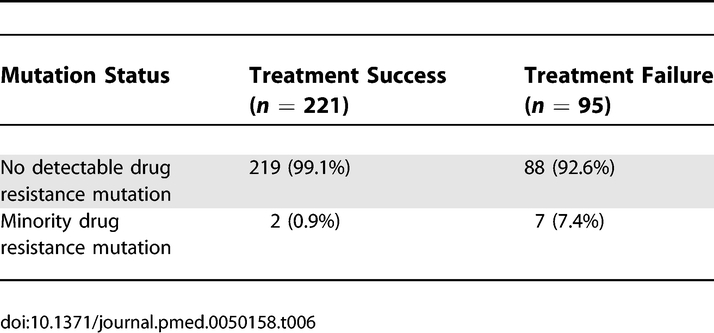
We performed a cross-sectional analysis of transmitted HIV-1 drug resistance and a case-control study of the impact of minority drug resistance on treatment response. For the cross-sectional analysis, we examined viral RNA from newly diagnosed ART-naïve persons in the US and Canada who had no detectable (wild type, n = 205) or one or more resistance-related mutations (n = 303) by conventional sequencing. Eight validated real-time PCR-based assays were used to test for minority drug resistance mutations (protease L90M and reverse transcriptase M41L, K70R, K103N, Y181C, M184V, and T215F/Y) above naturally occurring frequencies. The sensitive real-time PCR testing identified one to three minority drug resistance mutation(s) in 34/205 (17%) newly diagnosed persons who had wild-type virus by conventional genotyping; four (2%) individuals had mutations associated with resistance to two drug classes. Among 30/303 (10%) samples with bulk genotype resistance mutations we found at least one minority variant with a different drug resistance mutation. For the case-control study, we assessed the impact of three treatment-relevant drug resistance mutations at baseline from a separate group of 316 previously ART-naïve persons with no evidence of drug resistance on bulk genotype testing who were placed on efavirenz-based regimens. We found that 7/95 (7%) persons who experienced virologic failure had minority drug resistance mutations at baseline; however, minority resistance was found in only 2/221 (0.9%) treatment successes (Fisher exact test, p = 0.0038).
Conclusions
These data suggest that a considerable proportion of transmitted HIV-1 drug resistance is undetected by conventional genotyping and that minority mutations can have clinical consequences. With no treatment history to help guide therapies for drug-naïve persons, the findings suggest an important role for sensitive baseline drug resistance testing.
Since the mid-1990s, several powerful antiretroviral drug combinations have been developed that have greatly improved the prognosis of HIV infection. All antiretroviral therapy (ART) regimens combine drugs that act against HIV in different ways (so-called different drug classes). Multiple drugs are necessary because HIV continually accumulates random changes (mutations) in its genetic material (genome). Some of these mutations make HIV resistant to individual antiretroviral drugs, so a mixture of drugs is needed to keep the virus in check. However, the efficacy of ART (which itself selects for drug-resistant variants by giving them a growth advantage over drug-sensitive variants) is substantially reduced when these variants account for more than about 20% of the viruses in an infected person. This level of variant virus can be detected in blood samples with a technique called bulk sequencing. In North America and Europe, where ART has been widely used for many years, around 20% of HIV-infected people who have taken ART themselves develop this level of drug-resistant virus, which can be transmitted by the same routes as nonresistant HIV (typically unprotected sexual intercourse or needle sharing). In such cases, the person acquiring drug-resistant HIV may experience treatment failure when drugs later fail to work against the resistant virus. In these countries, therefore, resistance testing by bulk sequencing is done routinely before ART is initiated to decide which antiviral drugs are likely to be effective.
Why Was This Study Done?
Several years usually elapse between the time a person becomes infected with HIV and the time he or she starts ART. During this time, the absence of selection pressure from antiviral drugs means that transmitted drug-resistant variants tend to decline to levels undetectable by bulk sequencing. These “minority drug-resistant variants” can be detected using other more sensitive tests but it is not known what proportion of HIV-infected people who have never taken ART carry minority drug-resistant variants (the “prevalence” of these variants). It is also unknown whether the presence of minority drug-resistant variants reduces the success of ART. In this paper, the researchers first report a “cross-sectional” study in North America using a sensitive assay to determine the prevalence of minority drug-resistant viruses among HIV-infected people who had never received ART. They then investigate whether minority drug-resistant variants have any impact on the effectiveness of ART in a “case-control” study.
What Did the Researchers Do and Find?
In their cross-sectional study, the researchers used a highly sensitive test for detecting mutations (called a real-time PCR-based assay) to look for low levels of viruses carrying any of eight major drug-resistance mutations in people with newly diagnosed HIV infection who reported no prior treatment with ART. Seventeen percent of the people who had only wild-type (nonmutated) virus by bulk sequencing (205 participants) were found, in fact, to carry low levels of virus variants with 1–3 drug-resistance mutations; 2% of them carried viruses resistant to two different drug classes (called multi-drug resistance). Among the people with resistance mutations detected by bulk sequencing (303 participants), 10% had at least one additional minority drug-resistant variant, often a viral variant that was resistant to a drug class different from that detected by bulk sequencing. In the case-control study, the researchers used their sensitive assays to measure the levels of viruses containing any of the three most common drug resistance mutations likely to affect viral responses to the antiretroviral drugs efavirenz and lamivudine in 316 people just before they started their first HIV treatment, which included these drugs. Of people for whom ART failed, 7% were infected with minority drug-resistant virus variants at baseline compared with only 0.9% of people for whom ART worked; this difference was statistically significant.
What Do These Findings Mean?
The findings of the cross-sectional study indicate that conventional bulk sequencing fails to detect a large proportion of transmitted HIV drug resistance and suggest that the transmission of drug-resistant variants from infectious ART-experienced people to ART-naïve individuals might not be uncommon. The findings of the case-control study suggest that the minority drug-resistant HIV variants may have clinical consequences. That is, the presence of such variants in individuals who have not previously taken ART may reduce the efficacy of some ART regimens. However, the number of participants meeting the criteria for analysis in the cross-sectional study was limited, and the association between minority resistance and treatment failure may have been influenced by other factors. Taken together, these findings suggest that, to ensure that first-line ART is as effective as possible, greater efforts should be made to prevent HIV transmission, whether from ART-experienced or ART-naive people. However, because data on minority drug-resistant virus are limited, more studies— particularly with recent populations—are needed before testing for these variants can be considered appropriate in the clinical management of newly diagnosed HIV infection.
Additional Information.
Please access these Web sites via the online version of this summary at http://dx.doi.org/10.1371/journal.pmed.0050158.
-
Subjects:
-
Source:PLoS Med. 2008; 5(7).
-
Document Type:
-
Volume:5
-
Issue:7
-
Collection(s):
-
Main Document Checksum:urn:sha-512:4308ca16b2b36bd659b7db1e665058aab42b1d67a6ddd1ef67c7c94322870d769ebfa77a67e205f798c754a5ea47fe46d9172a27da691b7ba93dd155bd2f9a54
-
Download URL:
-
File Type:
 [PDF
- 338.69 KB
]
[PDF
- 338.69 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access