Systematic Review of the Effect of Pneumococcal Conjugate Vaccine Dosing Schedules on Vaccine-type Invasive Pneumococcal Disease Among Young Children
Supporting Files
Public Domain

-
Jan 2014
-
Details
-
Alternative Title:Pediatr Infect Dis J
-
Personal Author:
-
Description:Background:
Pneumococcal conjugate vaccines (PCV) are being implemented globally using a variety of different schedules. The optimal schedule to maximize protection of vaccinated children against vaccine-type invasive pneumococcal disease (VT-IPD) is not known.
Methods:
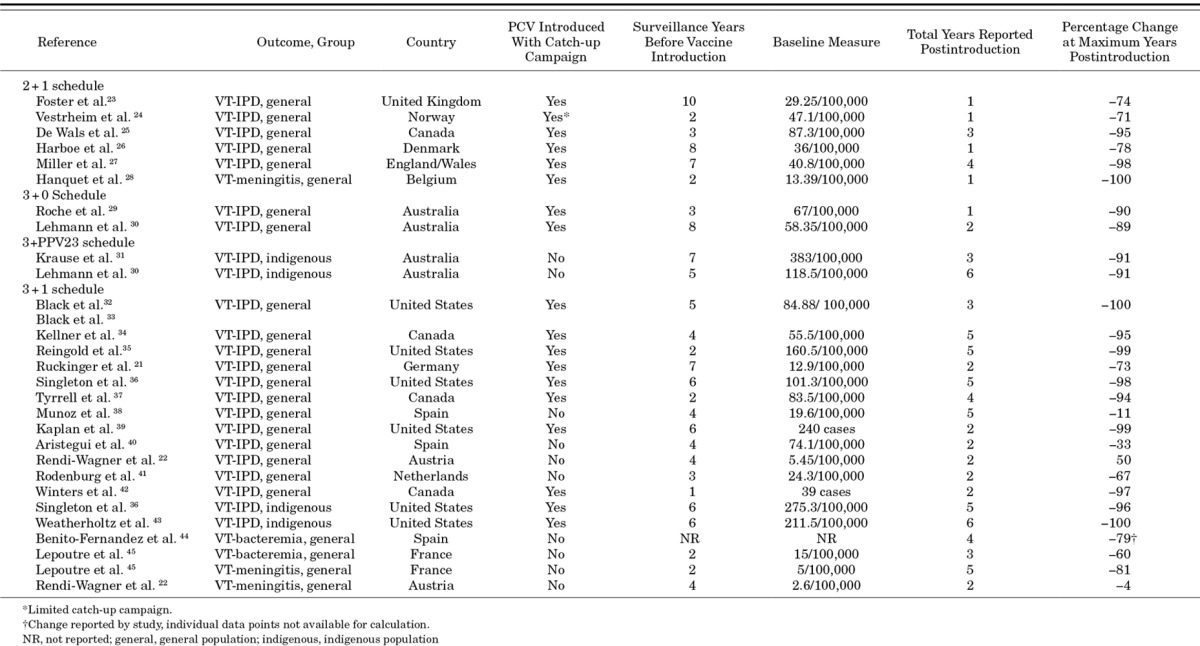
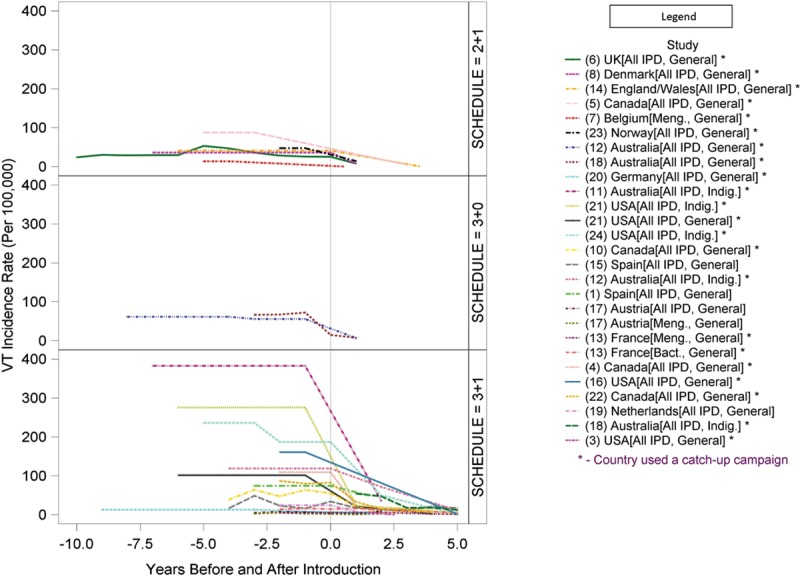
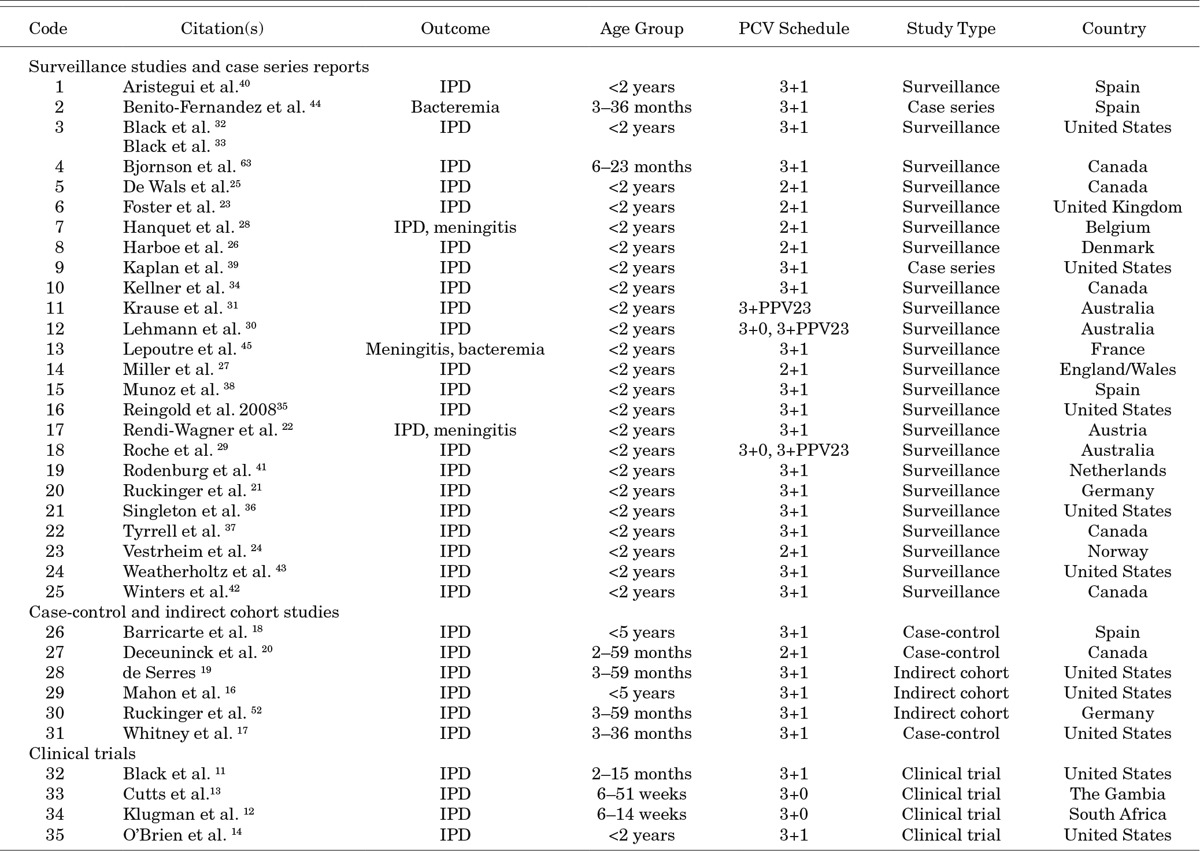
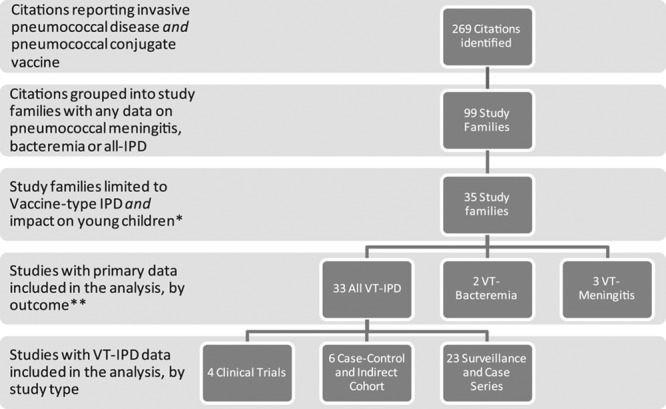
To assess the relative benefit of various PCV dosing schedules, we conducted a systematic review of studies published in English from 1994 to 2010 (supplemented post hoc with studies from 2011) on PCV effectiveness against VT-IPD among children targeted to receive vaccine. Data on 2-dose and 3-dose primary series, both with and without a booster (“2+0,” “2+1,” “3+0” and “3+1”), were included. For observational studies using surveillance data or case counts, we calculated percentage reduction in VT-IPD before and after PCV introduction.
Results:
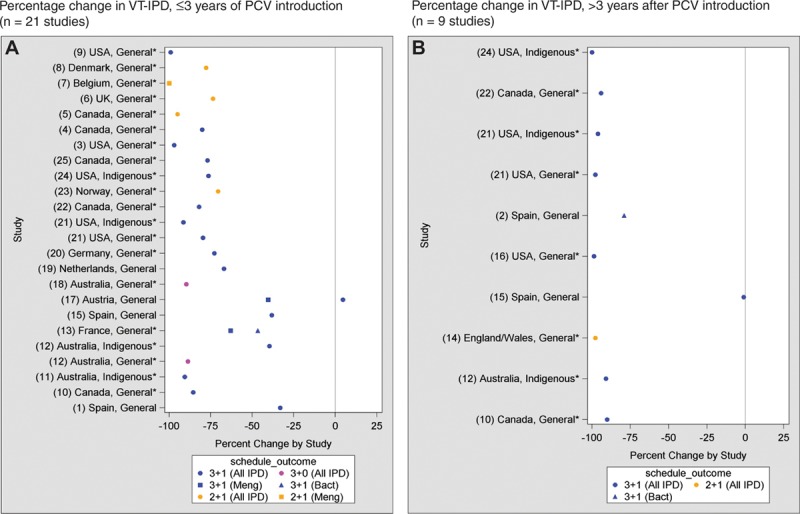
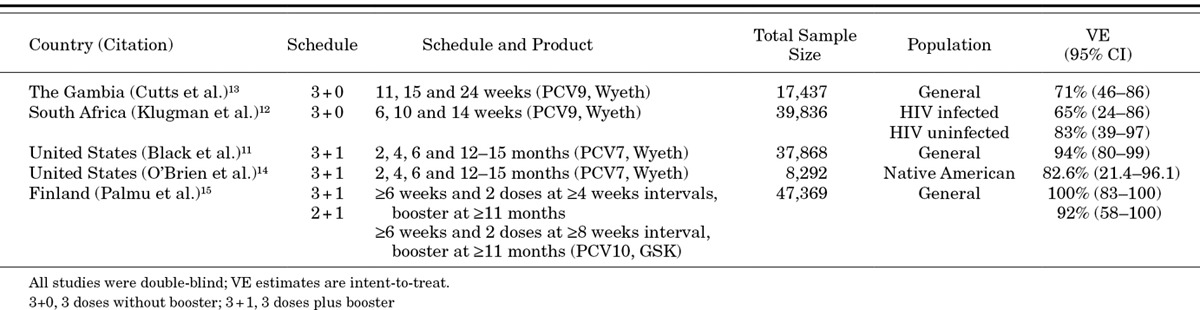
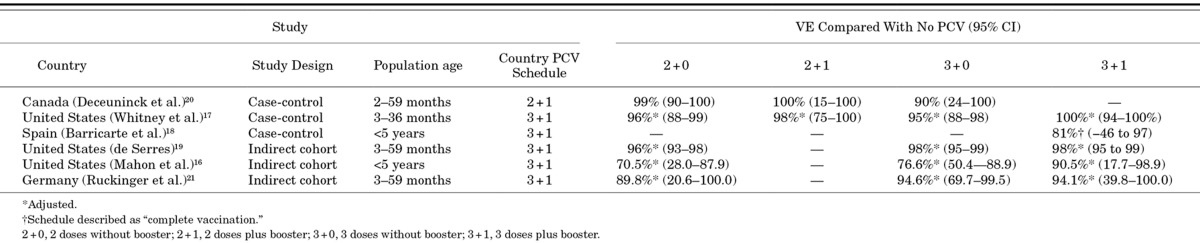
Of 4 randomized controlled trials and 31 observational studies reporting VT-IPD among young children, none evaluated a 2+0 complete series, 7 (19%) evaluated 2+1, 4 (11%) 3+0 and 27 (75%) 3+1. Most (86%) studies were from North America or Europe. Only 1 study (observational) directly compared 2 schedules (3+0 vs. 3+1); results supported the use of a booster dose. In clinical trials, vaccine efficacy ranged from 65% to 71% with 3+0 and 83% to 94% with 3+1. Surveillance data and case counts demonstrate reductions in VT-IPD of up to 100% with 2+1 (6 studies) or 3+1 (17 studies) schedules and up to 90% with 3+0 (2 studies). Reductions were observed as early as 1 year after PCV introduction.
Conclusions:
These data support the use of 2+1, 3+0 and 3+1 schedules, although most data of PCV impact on VT-IPD among young children are from high-income countries using 3+1. Differences between schedules for impact on VT-IPD are difficult to discern based on available data.
-
Subjects:
-
Source:Pediatr Infect Dis J. 2014; 33(Suppl 2 Optimum Dosing of Pneumococcal Conjugate Vaccine For Infants 0 A Landscape Analysis of Evidence Supportin g Different Schedules):S109-S118.
-
Document Type:
-
Volume:33
-
Collection(s):
-
Main Document Checksum:urn:sha256:2682df3643b9d2084b9edf668376acfb1483dba2d95dcb4213ff9b4353b9cab2
-
Download URL:
-
File Type:
 [PDF
- 1.27 MB
]
[PDF
- 1.27 MB
]
Supporting Files

ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access