
i
Risk Factors and Outcomes for Late Presentation for HIV-Positive Persons in Europe: Results from the Collaboration of Observational HIV Epidemiological Research Europe Study (COHERE)
-
Sep 03 2013
Source: PLoS Med. 2013; 10(9).
 [PDF-1.06 MB]
[PDF-1.06 MB]
Details:
-
Alternative Title:PLoS Med
-
Personal Author:
-
Corporate Authors:
-
Description:Amanda Mocroft and colleagues investigate risk factors and health outcomes associated with diagnosis at a late stage of infection in individuals across Europe.
Background
Few studies have monitored late presentation (LP) of HIV infection over the European continent, including Eastern Europe. Study objectives were to explore the impact of LP on AIDS and mortality.
Methods and Findings
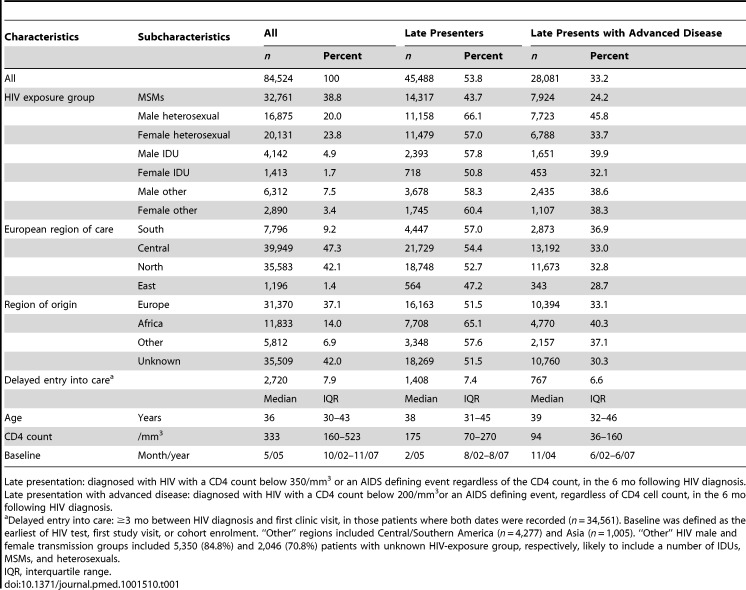
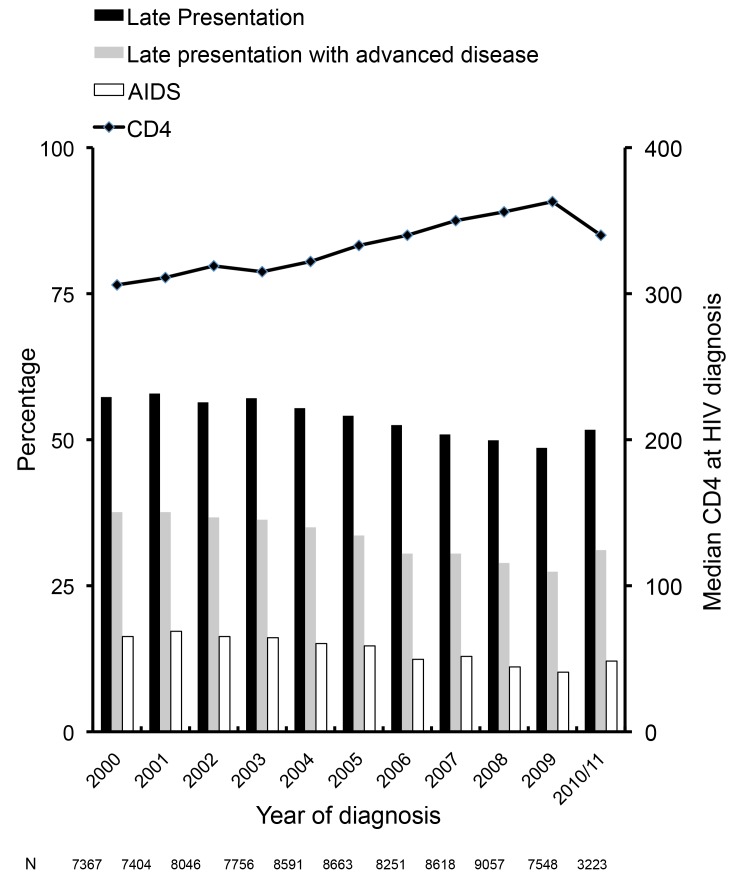
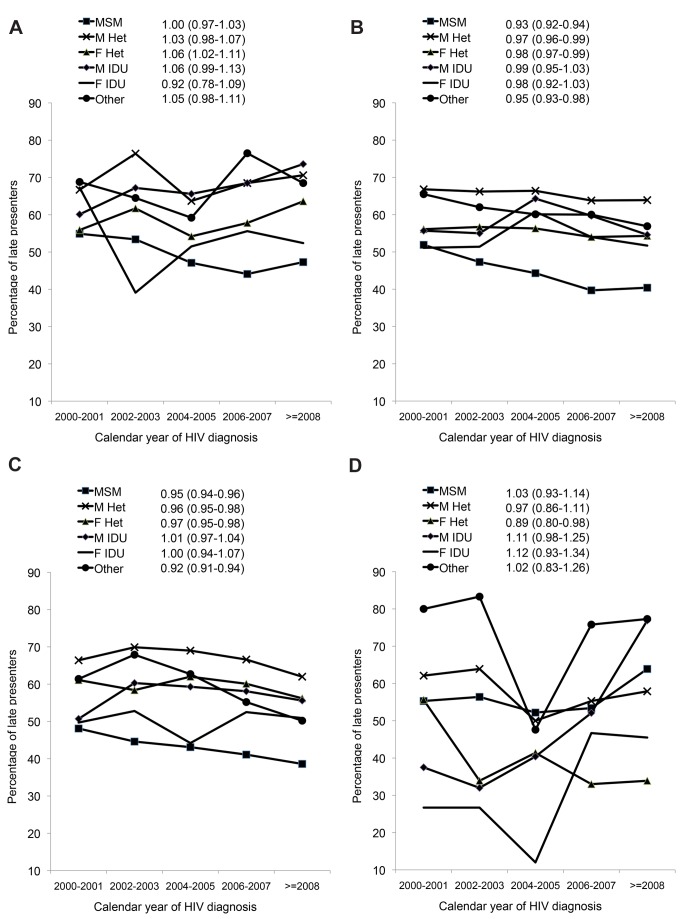
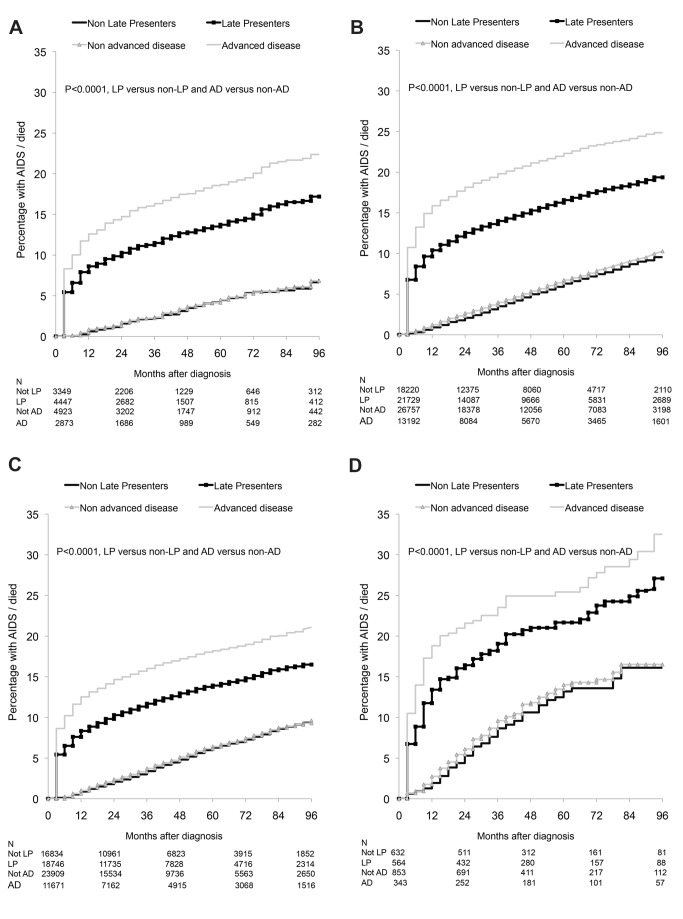
LP was defined in Collaboration of Observational HIV Epidemiological Research Europe (COHERE) as HIV diagnosis with a CD4 count <350/mm3 or an AIDS diagnosis within 6 months of HIV diagnosis among persons presenting for care between 1 January 2000 and 30 June 2011. Logistic regression was used to identify factors associated with LP and Poisson regression to explore the impact on AIDS/death. 84,524 individuals from 23 cohorts in 35 countries contributed data; 45,488 were LP (53.8%). LP was highest in heterosexual males (66.1%), Southern European countries (57.0%), and persons originating from Africa (65.1%). LP decreased from 57.3% in 2000 to 51.7% in 2010/2011 (adjusted odds ratio [aOR] 0.96; 95% CI 0.95–0.97). LP decreased over time in both Central and Northern Europe among homosexual men, and male and female heterosexuals, but increased over time for female heterosexuals and male intravenous drug users (IDUs) from Southern Europe and in male and female IDUs from Eastern Europe. 8,187 AIDS/deaths occurred during 327,003 person-years of follow-up. In the first year after HIV diagnosis, LP was associated with over a 13-fold increased incidence of AIDS/death in Southern Europe (adjusted incidence rate ratio [aIRR] 13.02; 95% CI 8.19–20.70) and over a 6-fold increased rate in Eastern Europe (aIRR 6.64; 95% CI 3.55–12.43).
Conclusions
LP has decreased over time across Europe, but remains a significant issue in the region in all HIV exposure groups. LP increased in male IDUs and female heterosexuals from Southern Europe and IDUs in Eastern Europe. LP was associated with an increased rate of AIDS/deaths, particularly in the first year after HIV diagnosis, with significant variation across Europe. Earlier and more widespread testing, timely referrals after testing positive, and improved retention in care strategies are required to further reduce the incidence of LP.
Every year about 2.5 million people become newly infected with HIV, the virus that causes AIDS. HIV can be transmitted through unprotected sex with an infected partner, from an HIV-positive mother to her unborn baby, or through injection of drugs. Most people do not become ill immediately after infection with HIV although some develop a short influenza-like illness. The next stage of the HIV infection, which may last up to 10 years, also has no major symptoms but, during this stage, HIV slowly destroys immune system cells, including CD4 cells, a type of lymphocyte. Eventually, when the immune system is unable to fight off infections by other disease-causing organisms, HIV-positive people develop AIDS-defining conditions—unusual viral, bacterial, and fungal infections and unusual tumors. Progression to AIDS occurs when any severe AIDS-defining condition is diagnosed, when the CD4 count in the blood falls below 200 cells/mm3, or when CD4 cells account for fewer than 15% of lymphocytes.
Why Was This Study Done?
People need to know they are HIV positive as soon as possible after they become infected because antiretroviral therapy, which controls but does not cure HIV infection, works best if it is initiated when people still have a relatively high CD4 count. Early diagnosis also reduces the risk of onward HIV transmission. However, 40%–60% of HIV-positive individuals in developed countries are not diagnosed until they have a low CD4 count or an AIDS-defining illness. Reasons for such late presentation include fear of discrimination or stigmatization, limited knowledge about HIV risk factors, testing, and treatment together with missed opportunities to offer an HIV test. Policy makers involved in national and international HIV control programs need detailed information about patterns of late presentation before they can make informed decisions about how to reduce this problem. In this study, therefore, the researchers use data collected by the Collaboration of Observational HIV Epidemiological Research in Europe (COHERE) to analyze trends in late presentation over time across Europe and in different groups of people at risk of HIV infection and to investigate the clinical consequences of late presentation.
What Did the Researchers Do and Find?
The researchers analyzed data collected from 84,524 individuals participating in more than 20 observational studies that were undertaken in 35 European countries and that investigated outcomes among HIV-positive people. Nearly 54% of the participants were late presenters—individuals who had a CD4 count of less than 350 cells/mm3 or an AIDS-defining illness within 6 months of HIV diagnosis. Late presentation was highest among heterosexual males, in Southern European countries, and among people originating in Africa. Overall, late presentation decreased from 57.3% in 2000 to 51.7% in 2010/11. However, whereas late presentation decreased over time among men having sex with men in Central and Northern Europe, for example, it increased over time among female heterosexuals in Southern Europe. Finally, among the 8,000 individuals who developed a new AIDS-defining illness or died during follow-up, compared to non-late presentation, late presentation was associated with an increased incidence of AIDS/death in all regions of Europe during the first and second year after HIV diagnosis (but not in later years); the largest increase in incidence (13-fold) occurred during the first year after diagnosis in Southern Europe.
What Do These Findings Mean?
These findings indicate that, although late presentation with HIV infection has decreased in recent years, it remains an important issue across Europe and in all groups of people at risk of HIV infection. They also show that individuals presenting late have a worse clinical outlook, particularly in the first and second year after diagnosis compared to non-late presenters. Several aspects of the study design may affect the accuracy and usefulness of these findings, however. For example, some of the study participants recorded as late presenters may have been people who were aware of their HIV status but who chose not to seek care for HIV infection, or may have been seen in the health care system prior to HIV diagnosis without being offered an HIV test. Delayed entry into care and late presentation are likely to have different risk factors, a possibility that needs to be studied further. Despite this and other study limitations, these findings nevertheless suggest that HIV testing strategies that encourage early testing in all populations at risk, that ensure timely referrals, and that improve retention in care are required to further reduce the incidence of late presentation with HIV infection in Europe.
Additional Information
Please access these websites via the online version of this summary at http://dx.doi.org/ 10.1371/journal.pmed.1001510.
-
Subjects:
-
Source:
-
Document Type:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
Supporting Files
-
docx
docx
docx
docx
docx 
gif 
jpeg 
gif 
jpeg 
gif 
txt 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg
txt









More +


 Email
CDC-INFO
Email
CDC-INFO









