Progress in Pediatric Asthma Surveillance I: The Application of Health Care Use Data in Alameda County, California
Supporting Files
Public Domain

-
Jun 15 2006
-
File Language:
English
Details
-
Journal Article:Preventing Chronic Disease (PCD)
-
Personal Author:
-
Description:Introduction
The ability to conduct community-level asthma surveillance is increasingly crucial for public health programming and child health advocacy. We explored the potential and limitations of health care use records from both public and private sources for asthma surveillance in a California county.
Methods
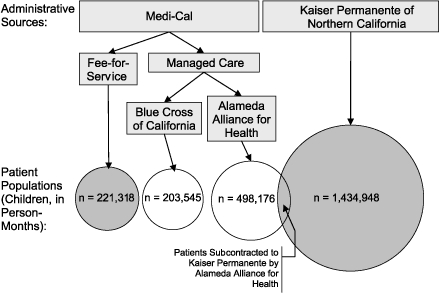
We combined administrative patient record data from Kaiser Permanente of Northern California and Medi-Cal (the California Medicaid program) for Alameda County residents during 2001. We assessed the resulting data set for completeness, population representation, consistency with external data, and internal indicator consistency.
Results
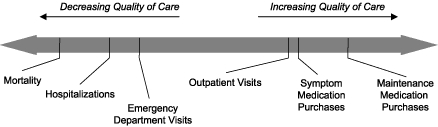
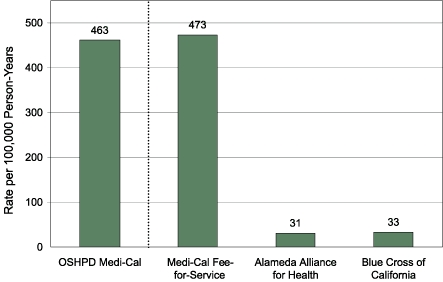
Our resulting data set included records for 226,383 children younger than 18 years. Completeness of Medicaid data was affected by managed care market share, reducing our usable data set size to 176,789, approximately equal to one of every two children in the county or one of every 3 person-months. External data documenting hospitalization rates due to asthma were poorly correlated with hospitalization rates (r = 0.2120, P = .20) but highly correlated with emergency department visits (r = 0.8607, P <.001) in the resulting data set. High internal consistency of indicators suggested that the data set represented a broad spectrum of health care access and quality of care congruent with clinical aspects of the disease.
Conclusion
The utility of these data is affected by logistical and administrative factors, including the health care payment structure and the market shares of care providers. These factors can be expected to similarly affect the utility of this approach in other counties. Our ability to generate county-level health statistics for comparison with other locations was limited, although the data set appeared well suited for within-county geographic analysis. In light of these findings, these data have the potential to expand the local health surveillance capacity of communities.
-
Subjects:
-
Source:Prev Chronic Dis. 2006; 3(3).
-
ISSN:1545-1151
-
Document Type:
-
Place as Subject:
-
Location:
-
Volume:3
-
Issue:3
-
Collection(s):
-
Main Document Checksum:urn:sha-512:002b74095b0a2f97b04868ff8bef713c1e1582ac034a3288bb332ec1e782e5361a2aab8b1ff27470654c8b6442d10697f7e695ec7b47163eb8f704b0ad282995
-
Download URL:
-
File Type:
 [PDF
- 314.51 KB
]
[PDF
- 314.51 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
Preventing Chronic Disease