Incidence and predictors of attrition from HIV treatment among adults living with HIV in high caseload facilities following implementation of universal test and treat strategy in Ethiopia: A prospective cohort study
Supporting Files

-
11-2024
-
File Language:
English
Details
-
Alternative Title:HIV Med
-
Personal Author:
-
Description:Background:
The introduction of universal test and treat (UTT) strategy has demonstrated a reduction in attrition in some low resource settings. UTT was introduced in Ethiopia in 2016. However, there is paucity of information in the magnitude and predictors of attrition from HIV treatment in Ethiopia. This study aims to assess the incidence and predictors of attrition from HIV treatment among adults living with HIV (PLHIV) in high caseload facilities following the implementation of universal test and treat strategy in Ethiopia from March 2019 to June 2020.
Methods:
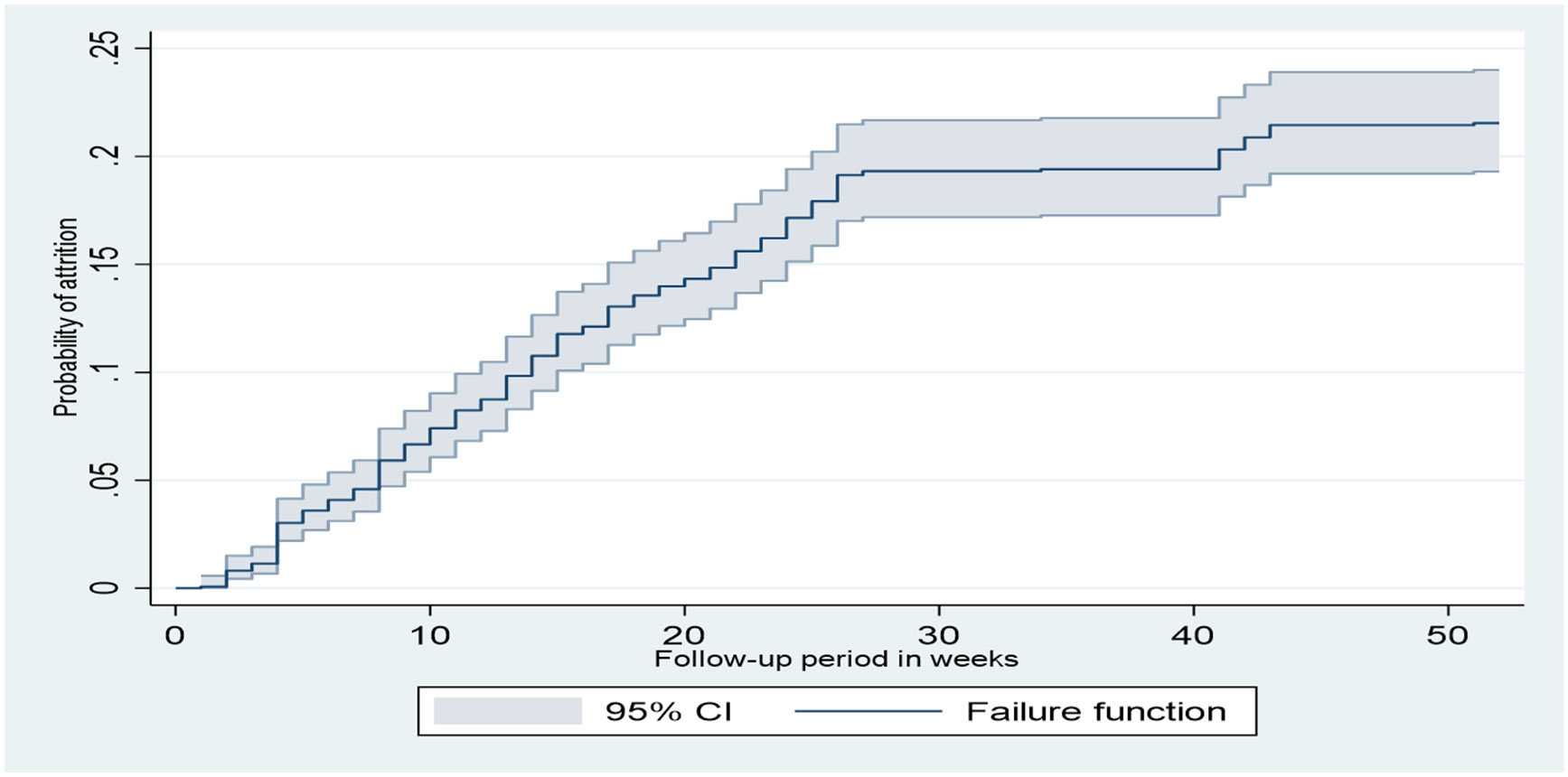
A prospective cohort of individuals in HIV care from 39 high case load facilities in Oromia, Amhara, Tigray, Addis Ababa and Dire Dawa regions of Ethiopia was conducted for 12 months. Participants were adults 15 year and older who were first testers recruited for three months from March to June 2019. Subsequent follow up was for 12 months, with data collected on sociodemographic and clinical conditions at baseline, six and 12 months and attrition at six and 12 months. We defined attrition as discontinuation from follow-up care due to lost to follow-up, dropout or death. Data were collected using Open Data Kit at field level and aggregated centrally. Kaplan-Meier survival analysis was employed to assess survival probability to the time of attrition from treatment. The Cox proportional hazard regression model was used to measure association of baseline predictor variables with the proportion of ART patients retained in ART during the follow up period.
Results:
The overall incidence rate for attrition from HIV treatment among the study participants during 12 months of follow-up was 5.02 cases per 1000 person-weeks (95% CI, 4.44-5.68 per 1000 person-weeks). Study participants from health facilities in Oromia and Addis Ababa/Dire Dawa had a 68%- and 51%- higher risk of attrition from HIV treatment compared to participants from Amhara region, respectively (adjusted hazard ratio (AHR) 1.68 95% CI (1.22-2.32), and AHR 1.51 95% CI (1.05-2.17), respectively). Participants who did not have a child had a 44% higher risk of attrition compared to those who had a child (AHR 1.44, 95% CI (1.12-1.85)). Individuals who did not own mobile phone had a 37% higher risk of attrition compared to those who owned mobile phone (AHR 1.37, 95% CI (1.02-1.83). Ambulatory/bedridden functional status at the time of diagnosis had a 44% higher risk of attrition compared to participants with a working functional status (AHR 1.44 95% CI (1.08-1.92)) at any time during the follow-up period.
Conclusion:
The overall incidence of attrition among people living with HIV enrolled in HIV treatment was not as high as what was reported by other studies. Independent predictors of attrition were administrative regions in Ethiopia where health facilities are located, not having a child, not owning mobile phone and being ambulatory/bedridden functional status at the time of diagnosis. Concerted efforts should be taken to reduce the magnitude of attrition from HIV treatment and address its drivers.
-
Subjects:
-
Keywords:
-
Source:HIV Med. 25(11):1227-1239
-
Pubmed ID:39107614
-
Pubmed Central ID:PMC11560704
-
Document Type:
-
Funding:
-
Volume:25
-
Issue:11
-
Collection(s):
-
Main Document Checksum:urn:sha-512:afd5201b7f3c776432cbe07fd8c90855fec1e26f52864e0999ff38983e0e21936d31aeb3ab857806c3fed4d60d320e05e87faca0fdb9fb66dec2930c4fa84d09
-
Download URL:
-
File Type:
 [PDF
- 630.23 KB
]
[PDF
- 630.23 KB
]
Supporting Files

File Language:
English

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access