Evaluation of a National Care Coordination Program to Reduce Utilization among High-cost, High-need Medicaid Beneficiaries with Diabetes
Supporting Files

-
6 2020
-
File Language:
English
Details
-
Alternative Title:Med Care
-
Personal Author:
-
Description:Background:
Medical, behavioral, and social determinants of health are each associated with high levels of emergency department (ED) visits and hospitalizations.
Objective:
To evaluate a care coordination program designed to provide combined “whole-person care,” integrating medical, behavioral and social support for high-cost, high-need Medicaid beneficiaries by targeting access barriers and social determinants.
Research Design:
Individual-level interrupted time series with a comparator group, using person-month as the unit of analysis.
Subjects:
42,214 UnitedHealthcare Medicaid beneficiaries (194,834 person-months) age ≥21 with diabetes, with Temporary Assistance to Needy Families (TANF), Medicaid expansion, Supplemental Security Income (SSI) without Medicare, or dual Medicaid/Medicare.
Measures:
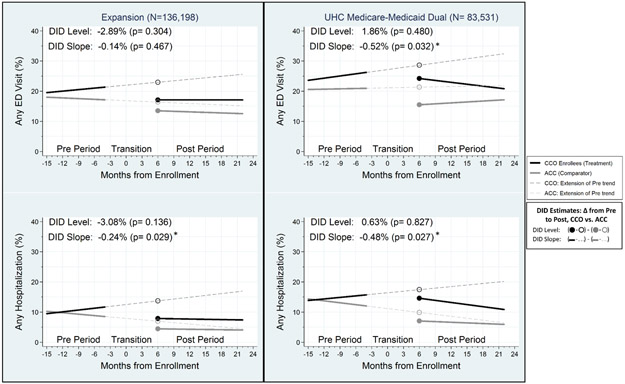
Our outcome measures were any hospitalizations and any ED visits in a given month. Covariates of interest included an indicator for intervention versus comparator group and indicator and spline variables measuring changes in an outcome’s time trend after program enrollment.
Results:
Overall, 6 of the 8 examined comparisons were not statistically significant. Among SSI beneficiaries, we observed a larger projected decrease in ED visit risk among the intervention sample versus the comparator sample at 12 months post enrollment (difference-in-difference/DID: −6.6%; 95% CI: −11.2%, −2.1%). Among expansion beneficiaries, we observed a greater decrease in hospitalization risk among the intervention sample versus the comparator sample at 12 months post enrollment (DID: −5.8%; 95% CI: −11.4%, −0.2%).
Conclusions:
A care coordination program designed to reduce utilization among high-cost, high-need Medicaid beneficiaries was associated with fewer ED visits and hospitalizations for patients with diabetes in selected Medicaid programs but not others.
-
Keywords:
-
Source:Med Care. 58(Suppl 6 1):S14-S21
-
Pubmed ID:32412949
-
Pubmed Central ID:PMC10653047
-
Document Type:
-
Funding:
-
Volume:58
-
Collection(s):
-
Main Document Checksum:urn:sha256:8a84c38df114926505a338927b52edf16a255f5c41c615758cbbc419ea87ac71
-
Download URL:
-
File Type:
 [PDF
- 426.51 KB
]
[PDF
- 426.51 KB
]

File Language:
English

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access