Trends and Factors Associated with Hospitalization Costs for Inflammatory Bowel Disease in the United States
Supporting Files

-
2 2019
-
File Language:
English
Details
-
Alternative Title:Appl Health Econ Health Policy
-
Personal Author:
-
Description:Background
Few studies have addressed recent trends in hospitalization costs for inflammatory bowel disease (IBD).
Objective
We explored trends and described patient and hospital factors associated with hospitalization costs for IBD.
Methods
Using data from the 2003–2014 National Inpatient Sample for adults aged ≥ 18 years, we estimated costs using multivariable linear models and assessed linear trends by time periods using piecewise linear regressions.
Results
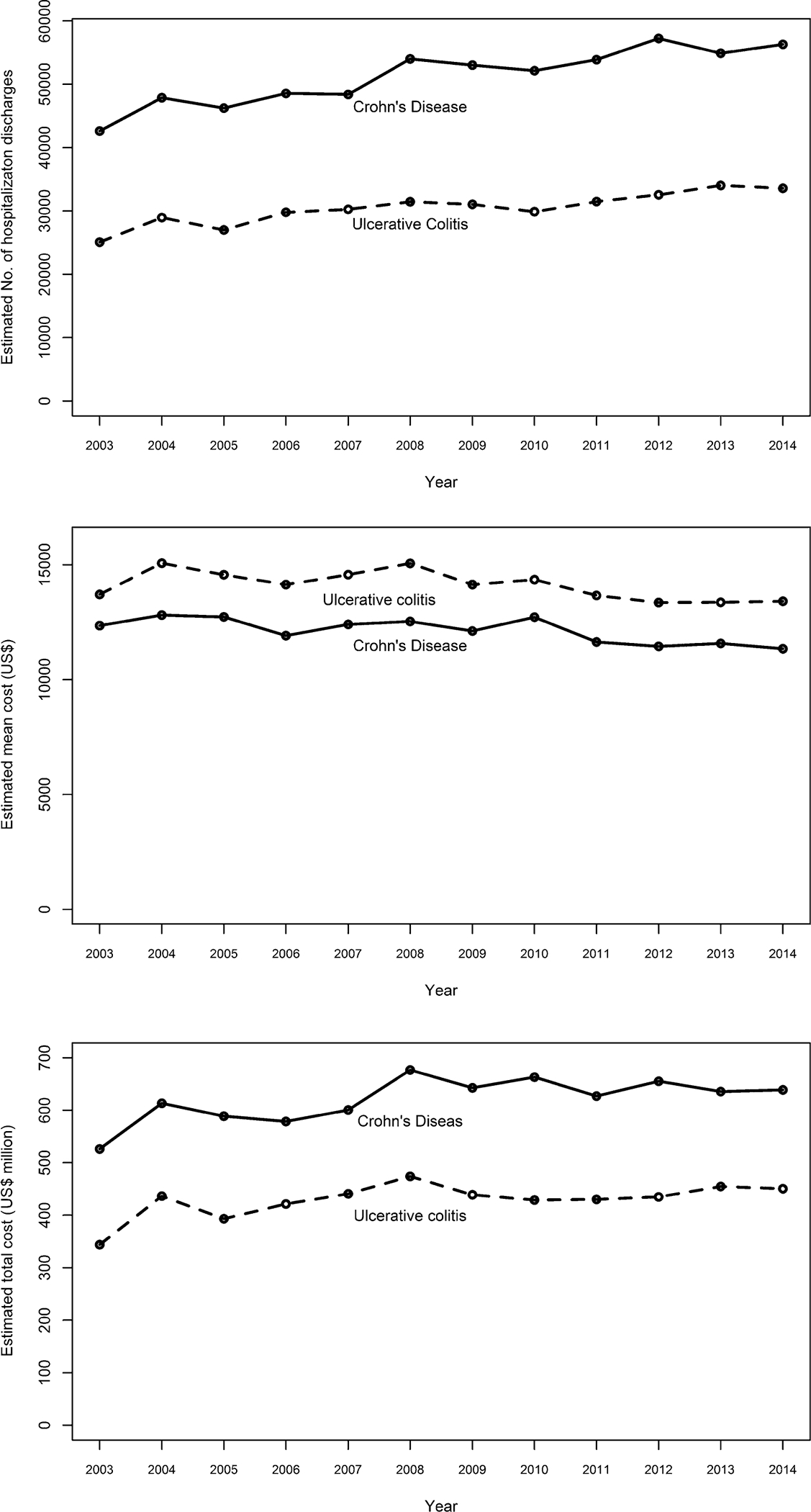
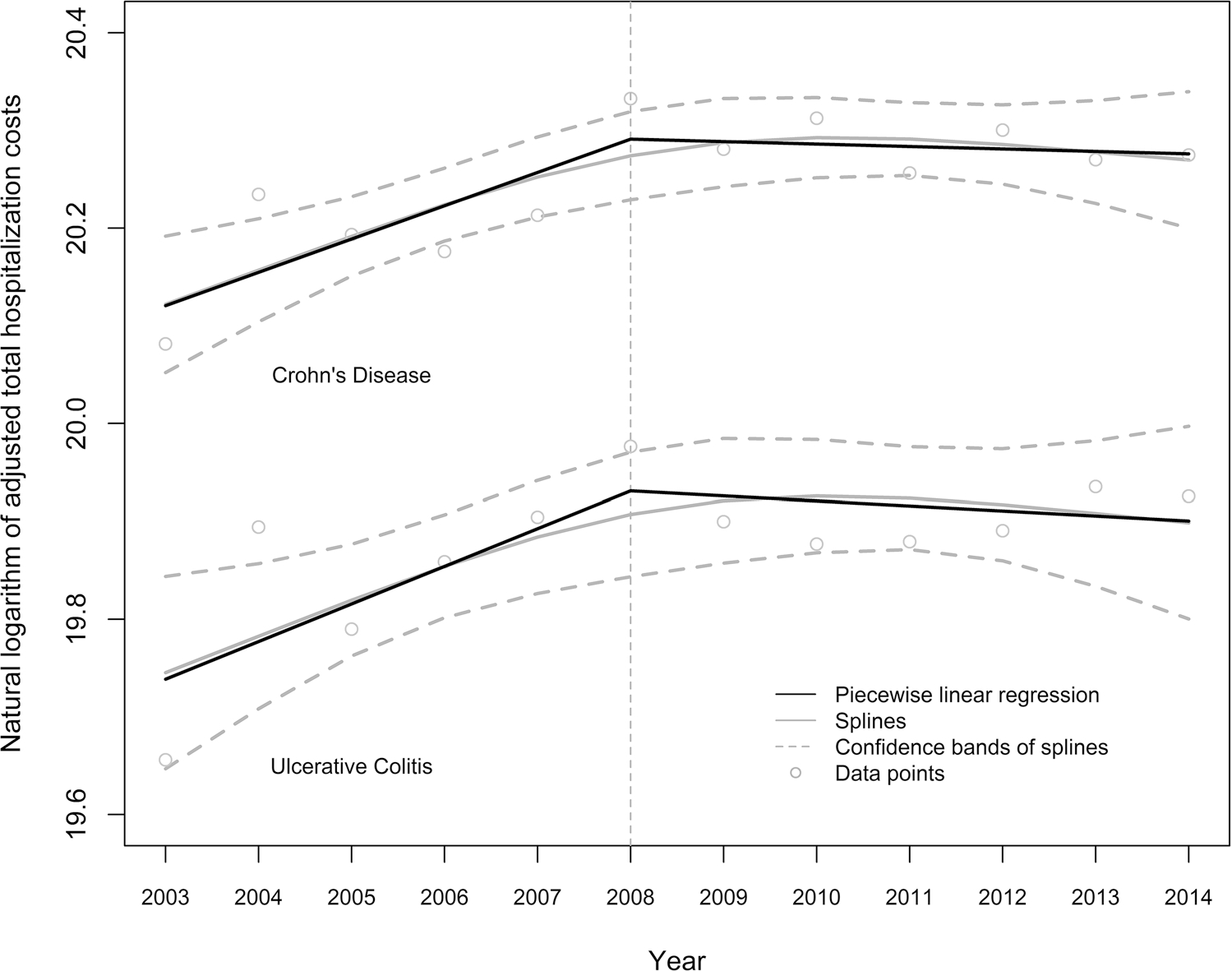
In 2014, there were an estimated 56,290 hospitalizations for Crohn’s disease (CD), with a mean cost of US$11,345 and median cost of US$7592; and 33,585 hospitalizations for ulcerative colitis (UC), with a mean cost of US$13,412 and median cost of US$8873. Higher costs were observed among Hispanic [adjusted cost ratio (ACR) = 1.07; 95% confidence interval (CI) = 1.00–1.14; p = 0.04] or other non-Hispanic (ACR = 1.09; 95% CI = 1.02–1.17; p = 0.01) CD patients than for non-Hispanic White CD patients. For UC patients, higher costs were observed among men (ACR = 1.09; 95% CI = 1.05–1.13; p < 0.001) compared with women and among patients aged 35–44 years, 45–54 years, and 55–64 years compared with those aged 18–24 years. Among all patients, factors associated with higher costs included higher household income, more comorbidities, and hospitals that were government nonfederal versus private, were large versus small, and were located in the West versus Northeast regions. From 2003 to 2008, total costs increased annually by 3% for CD (1.03; 95% CI = 1.02–1.05; p < 0.001) and 4% for UC (1.04; 95% CI = 1.02–1.06; p < 0.001), but remained unchanged from 2008 to 2014.
Conclusions
The findings are important to identify IBD patients with higher hospitalization costs and to inform policy plans on hospital resource allocation.
-
Subjects:
-
Source:Appl Health Econ Health Policy. 17(1):77-91
-
Pubmed ID:30259396
-
Pubmed Central ID:PMC10498392
-
Document Type:
-
Funding:
-
Place as Subject:
-
Volume:17
-
Issue:1
-
Collection(s):
-
Main Document Checksum:urn:sha256:bee9fbcf5a97cdc9267b9668081c7153da29409298d4c1c883a5da1f0ccba868
-
Download URL:
-
File Type:
 [PDF
- 511.29 KB
]
[PDF
- 511.29 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access