Cost-effectiveness of carbapenem-resistant Enterobacteriaceae (CRE) surveillance in Maryland
Supporting Files

File Language:
English
Details
-
Alternative Title:Infect Control Hosp Epidemiol
-
Personal Author:
-
Description:Objective:
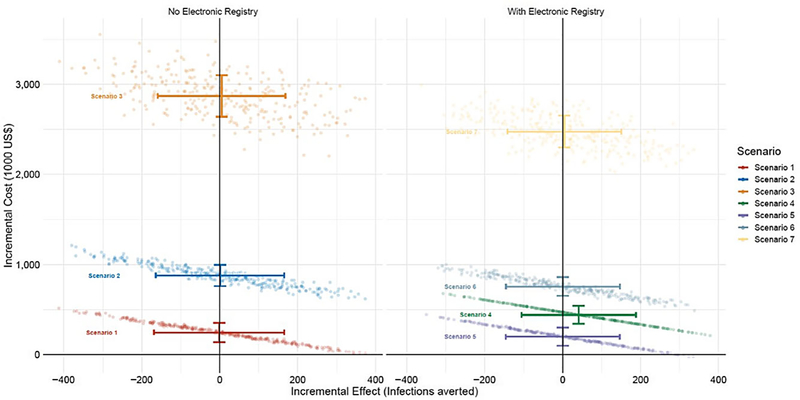
We analyzed the efficacy, cost, and cost-effectiveness of predictive decision-support systems based on surveillance interventions to reduce the spread of carbapenem-resistant Enterobacteriaceae (CRE).
Design:
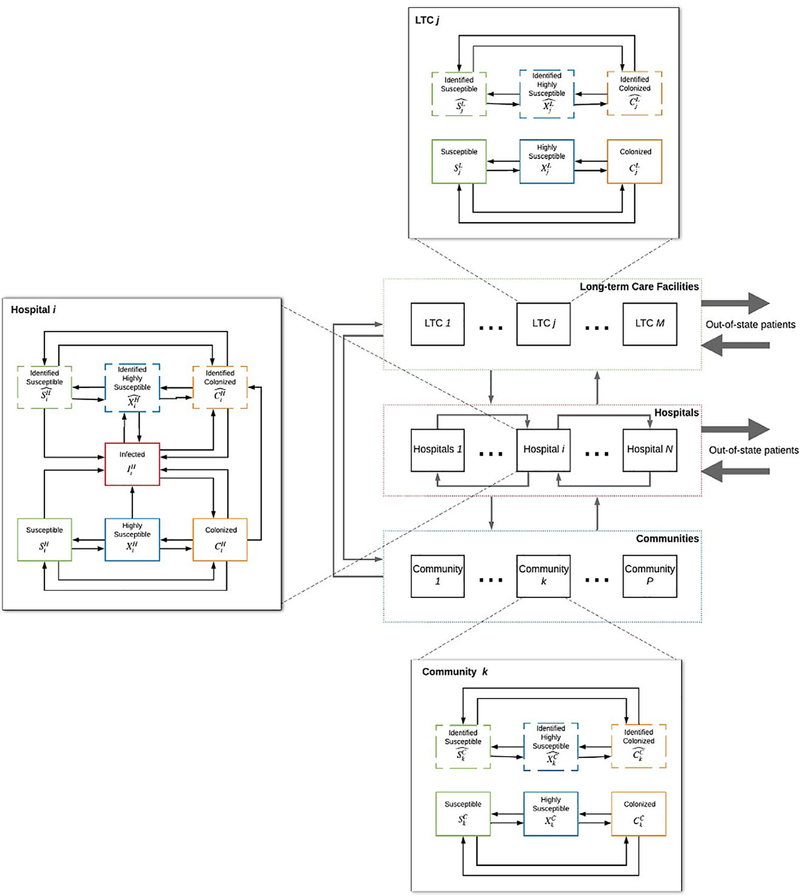
We developed a computational model that included patient movement between acute-care hospitals (ACHs), long-term care facilities (LTCFs), and communities to simulate the transmission and epidemiology of CRE. A comparative cost-effectiveness analysis was conducted on several surveillance strategies to detect asymptomatic CRE colonization, which included screening in ICUs at select or all hospitals, a statewide registry, or a combination of hospital screening and a statewide registry.
Setting:
We investigated 51 ACHs, 222 LTCFs, and skilled nursing facilities, and 464 ZIP codes in the state of Maryland.
Patients or participants:
The model was informed using 2013–2016 patient-mix data from the Maryland Health Services Cost Review Commission. This model included all patients that were admitted to an ACH.
Results:
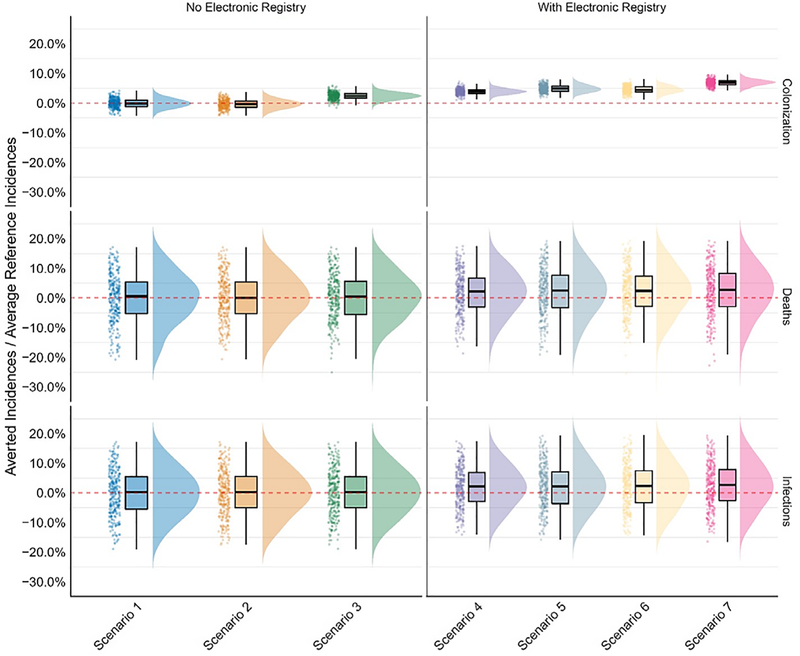
On average, the implementation of a statewide CRE registry reduced annual CRE infections by 6.3% (18.8 cases). Policies of screening in select or all ICUs without a statewide registry had no significant impact on the incidence of CRE infections. Predictive algorithms, which identified any high-risk patient, reduced colonization incidence by an average of 1.2% (3.7 cases) without a registry and 7.0% (20.9 cases) with a registry. Implementation of the registry was estimated to save $572,000 statewide in averted infections per year.
Conclusions:
Although hospital-level surveillance provided minimal reductions in CRE infections, regional coordination with a statewide registry of CRE patients reduced infections and was cost-effective.
-
Subjects:
-
Source:Infect Control Hosp Epidemiol. :1-9
-
Pubmed ID:34674791
-
Pubmed Central ID:PMC9023597
-
Document Type:
-
Funding:
-
Collection(s):
-
Main Document Checksum:urn:sha-512:9e10a992888848265881a8f534c77852a1d34349b969ab45fe9d4b59df7f762efe8f8d78e594411219742f092b5ca35416a898fd769aaa7491edb9fafc95fce6
-
Download URL:
-
File Type:
 [PDF
- 1000.14 KB
]
[PDF
- 1000.14 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access