Variation in initiation, engagement, and retention on medications for opioid use disorder based on health insurance plan design
Supporting Files

-
3 01 2022
-
File Language:
English
Details
-
Alternative Title:Med Care
-
Personal Author:
-
Description:Background:
The association between cost-sharing and receipt of medication for opioid use disorder (MOUD) is unknown.
Methods:
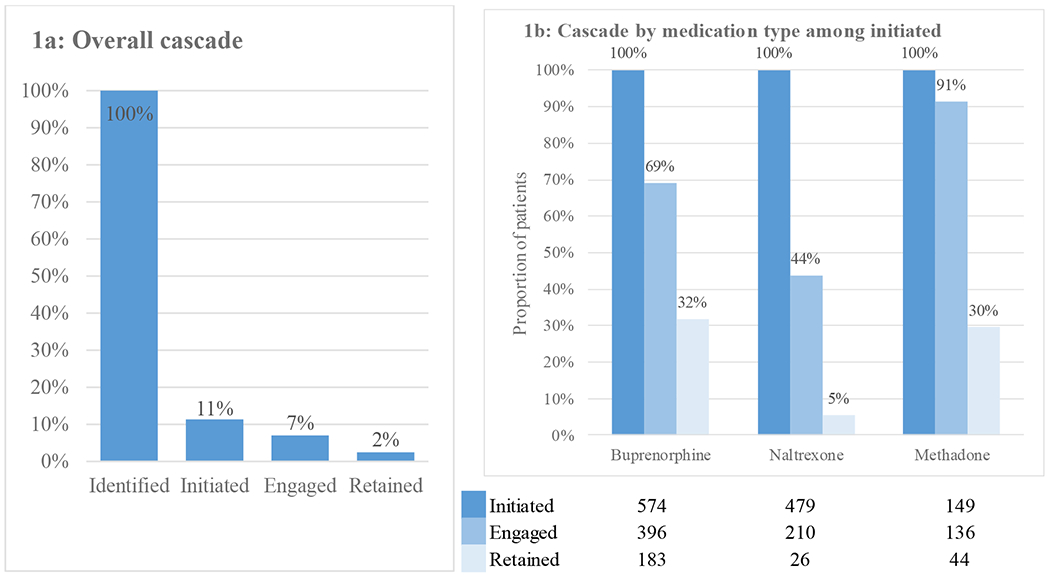
We constructed a cohort of 10,513 commercially insured individuals with a new diagnosis of opioid use disorder (OUD) and information on insurance cost-sharing in a large national de-identified claims database. We examined four cost-sharing measures: 1) pharmacy deductible; 2) medical service deductible; 3) pharmacy medication co-pay; and 4) medical office co-pay. We measured MOUD (naltrexone, buprenorphine, or methadone) initiation (within 14 days of diagnosis), engagement (second receipt within 34 days of first), and 6-month retention (continuous receipt without 14-day gap). We used multivariable logistic regression to assess the association between cost-sharing and MOUD initiation, engagement, and retention. We calculated total out-of-pocket costs in the 30 days following MOUD initiation for each type of MOUD.
Results:
Of 10,513 individuals with incident OUD, 1,202 (11%) initiated MOUD, 742 (7%) engaged, and 253 (2%) were retained in MOUD at six months. A high ($1,000+) medical deductible was associated with a lower odds of initiation compared to no deductible (odds ratio: 0.85, 95% CI: 0.74-0.98). We found no significant associations between other cost-sharing measures for initiation, engagement, or retention. Median initial 30-day out-of-pocket costs ranged from $100 for methadone to $710 for extended-release naltrexone.
Conclusion:
Among insurance plan cost-sharing measures, only medical services deductible showed an association with decreased MOUD initiation. Policy and benefit design should consider ways to reduce cost barriers to initiation and retention in MOUD.
-
Subjects:
-
Source:Med Care. 60(3):256-263
-
Pubmed ID:35026792
-
Pubmed Central ID:PMC8852217
-
Document Type:
-
Funding:
-
Volume:60
-
Issue:3
-
Collection(s):
-
Main Document Checksum:urn:sha256:98fa54a282f4bbea4cebec93eca4acd3e7167fe0b4d13c52f8cb39a894fffc19
-
Download URL:
-
File Type:
 [PDF
- 175.30 KB
]
[PDF
- 175.30 KB
]

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access