Morbidity and Mortality Weekly Report (MMWR): Surveillance Summaries, September 2019 / Vol. 68 / No. SS-8
Supporting Files
Public Domain

-
September 27, 2019
-
File Language:
English
Details
-
Alternative Title:Population-Based Active Surveillance for Culture-Confirmed Candidemia — Four Sites, United States, 2012–2016
-
Journal Article:Morbidity and Mortality Weekly Report (MMWR): Surveillance Summaries
-
Personal Author:
-
Corporate Authors:Center for Surveillance, Epidemiology, and Laboratory Services (U.S.) ; Division of Scientific Education and Professional Development ; Epidemic Intelligence Service ; National Center for Emerging and Zoonotic Infectious Diseases (U.S.). Division of Foodborne, Waterborne, and Environmental Diseases ; Emory University School of Medicine. Dept. of Medicine ; Atlanta Veterans Affairs Medical Center ; Johns Hopkins Bloomberg School of Public Health. Maryland Emerging Infections Program ; Oregon Health Authority ; Vanderbilt University School of Medicine
-
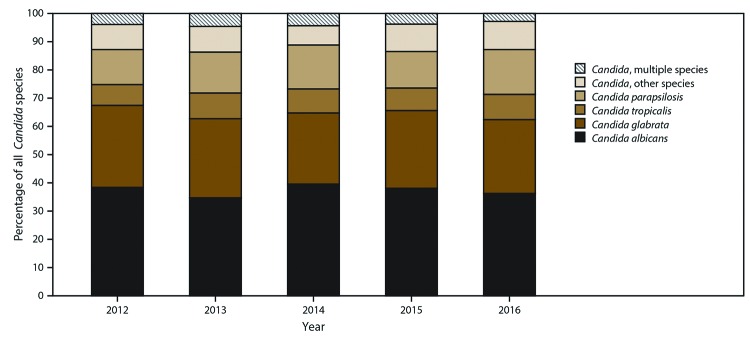
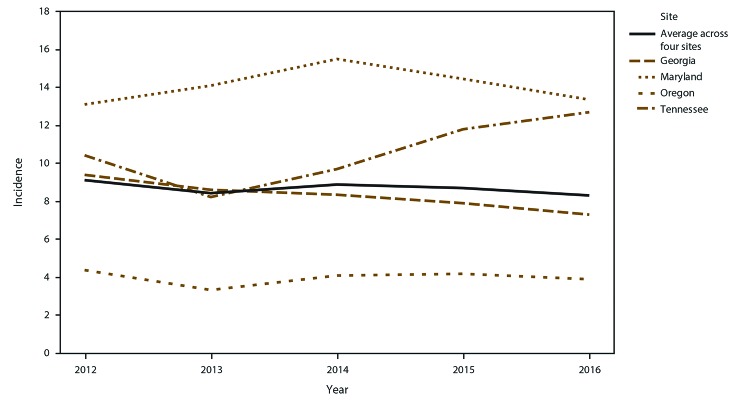
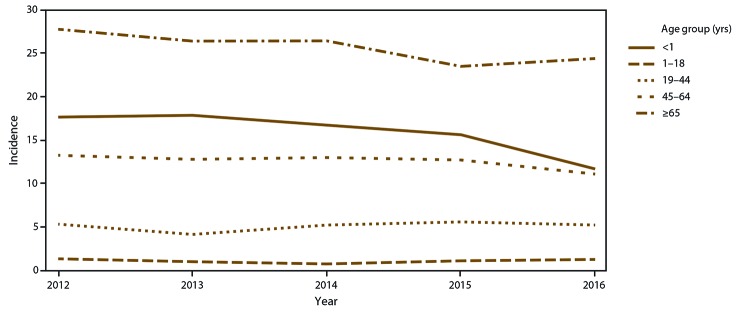
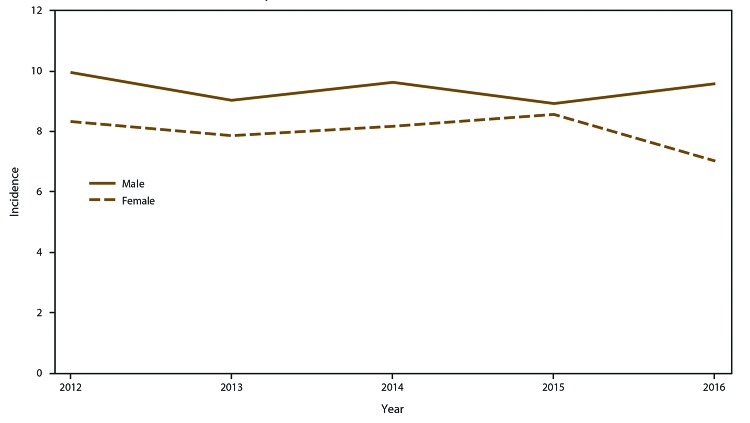
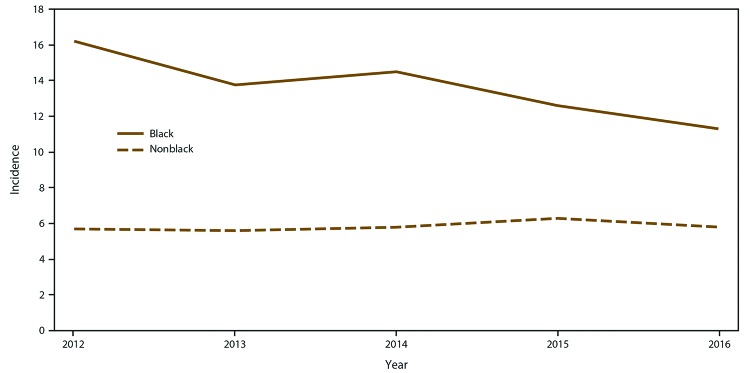
Description:Candidemia is a bloodstream infection (BSI) caused by yeasts in the genus Candida. Candidemia is one of the most common health care–associated BSIs in the U.S. with all-cause in-hospital Mortality of up to 30%. CDC’s Emerging Infections Program (EIP), a collaboration among CDC, state health departments, and academic partners that was established in 1995, was used to conduct active, population-based laboratory surveillance for candidemia in 22 counties in four states (Georgia, Maryland, Oregon, and Tennessee) with a combined population of approximately 8 million persons. Laboratories serving the catchment areas were recruited to report candidemia cases to the local EIP program staff. A case was defined as a blood culture that was positive for a Candida species collected from a surveillance area resident during 2012–2016. Isolates were sent to CDC for species confirmation and antifungal susceptibility testing. Any subsequent blood cultures with Candida within 30 days of the initial positive culture in the same patient were considered part of the same case. Trained surveillance officers collected clinical information from the medical chart for all cases, and isolates were sent to CDC for species confirmation and antifungal susceptibility testing.
Approximately nine out of 100,000 persons developed culture-positive candidemia annually in four U.S. sites. The youngest and oldest persons, men, and blacks had the highest incidences of candidemia. Patients with candidemia identified in the surveillance program had many of the typical risk factors for candidemia, including recent surgery, exposure to broad-spectrum antibiotics, and presence of a CVC. However, an unexpectedly high proportion of candidemia cases (10%) occurred in patients with a history of injection drug use (IDU), suggesting that IDU has become a common risk factor for candidemia. Deaths associated with candidemia remain high, with one in four cases resulting in death during hospitalization.
-
Subjects:
-
Source:Morbidity and Mortality Weekly Report (MMWR): Surveillance Summaries, 2019; v. 68, no. 8
-
Series:
-
DOI:
-
ISSN:1546-0738 (print) ; 1545-8636 (digital)
-
Pubmed ID:31557145
-
Pubmed Central ID:PMC6772189
-
Document Type:
-
Place as Subject:
-
Pages in Document:20 pdf pages
-
Volume:68
-
Issue:8
-
Collection(s):
-
Main Document Checksum:urn:sha-512:5263b47ed664df7059af13f885641c070f2090a4ba0a063f58571d12922467dd283f1555e31321a6d87e89f4cccfea7320f6a8d1296677cb3056d7e90585a8ff
-
Download URL:
-
File Type:
 [PDF
- 801.70 KB
]
[PDF
- 801.70 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
Morbidity and Mortality Weekly Report (MMWR)