Medication for Opioid Use Disorder After Nonfatal Opioid Overdose and Association With Mortality
Supporting Files

-
June 19 2018
-
File Language:
English
Details
-
Alternative Title:Ann Intern Med
-
Personal Author:
-
Description:Background:
Opioid overdose survivors have an increased risk for death. Whether use of medications for opioid use disorder (MOUD) after overdose is associated with mortality is not known.
Objective:
To identify MOUD use after opioid overdose and its association with all-cause and opioid-related mortality.
Design:
Retrospective cohort study.
Setting:
7 individually linked data sets from Massachusetts government agencies.
Participants:
17 568 Massachusetts adults without cancer who survived an opioid overdose between 2012 and 2014.
Measurements:
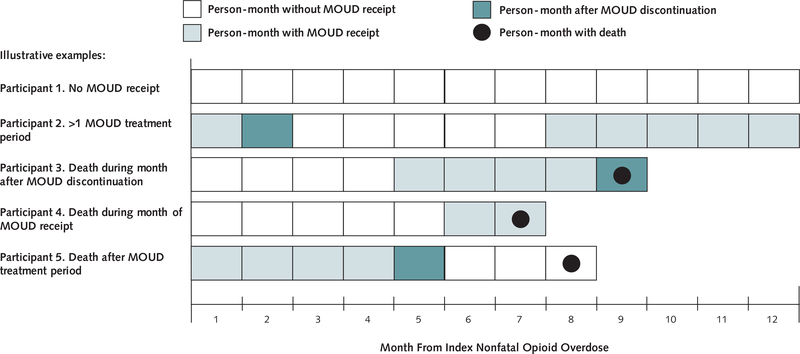
Three types of MOUD were examined: methadone maintenance treatment (MMT), buprenorphine, and naltrexone. Exposure to MOUD was identified at monthly intervals, and persons were considered exposed through the month after last receipt. A multivariable Cox proportional hazards model was used to examine MOUD as a monthly time-varying exposure variable to predict time to all-cause and opioid-related mortality.
Results:
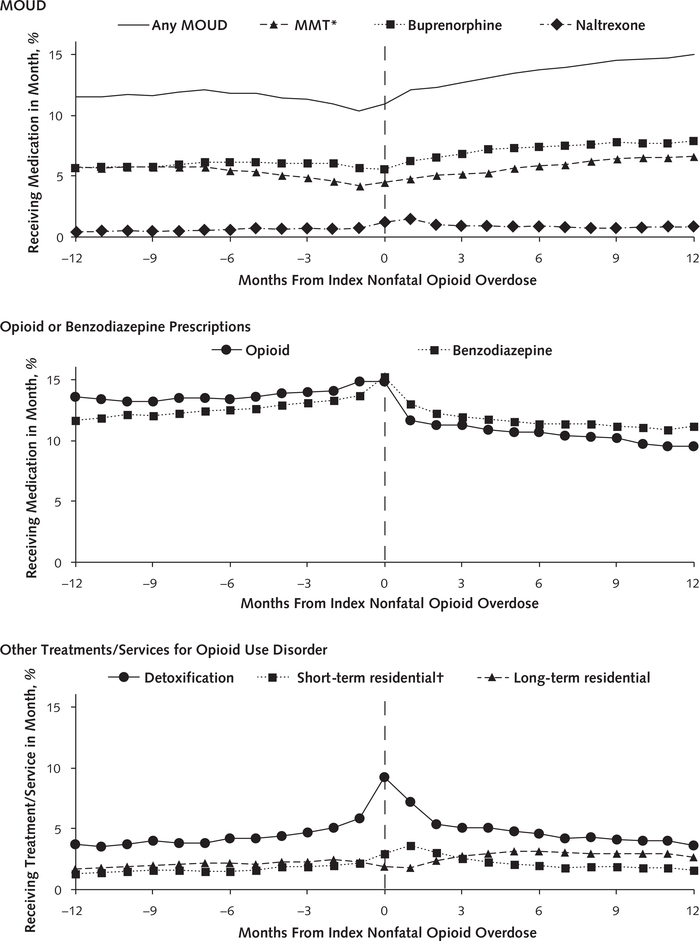
In the 12 months after a nonfatal overdose, 2040 persons (11%) enrolled in MMT for a median of 5 months (interquartile range, 2 to 9 months), 3022 persons (17%) received buprenorphine for a median of 4 months (interquartile range, 2 to 8 months), and 1099 persons (6%) received naltrexone for a median of 1 month (interquartile range, 1 to 2 months). Among the entire cohort, all-cause mortality was 4.7 deaths (95% CI, 4.4 to 5.0 deaths) per 100 person-years and opioid-related mortality was 2.1 deaths (CI, 1.9 to 2.4 deaths) per 100 person-years. Compared with no MOUD, MMT was associated with decreased all-cause mortality (adjusted hazard ratio [AHR], 0.47 [CI, 0.32 to 0.71]) and opioid-related mortality (AHR, 0.41 [CI, 0.24 to 0.70]). Buprenorphine was associated with decreased all-cause mortality (AHR, 0.63 [CI, 0.46 to 0.87]) and opioid-related mortality (AHR, 0.62 [CI, 0.41 to 0.92]). No associations between naltrexone and all-cause mortality (AHR, 1.44 [CI, 0.84 to 2.46]) or opioid-related mortality (AHR, 1.42 [CI, 0.73 to 2.79]) were identified.
Limitation:
Few events among naltrexone recipients preclude confident conclusions.
Conclusion:
A minority of opioid overdose survivors received MOUD. Buprenorphine and MMT were associated with reduced all-cause and opioid-related mortality.
Primary Funding Source:
National Center for Advancing Translational Sciences of the National Institutes of Health.
-
Subjects:
-
Source:Ann Intern Med. 169(3):137-145
-
Pubmed ID:29913516
-
Pubmed Central ID:PMC6387681
-
Document Type:
-
Funding:
-
Volume:169
-
Issue:3
-
Collection(s):
-
Main Document Checksum:urn:sha256:27202ece746515d708fd6d288f7a218bd10cea7d76f94cf8a560f4cd13ec207f
-
Download URL:
-
File Type:
 [PDF
- 928.39 KB
]
[PDF
- 928.39 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access