First 100 Persons with COVID-19 — Zambia, March 18–April 28, 2020
Supporting Files
Public Domain

-
October 23 2020
-
File Language:
English
Details
-
Journal Article:Morbidity and Mortality Weekly Report (MMWR)
-
Personal Author:Chipimo, Peter J. ; Barradas, Danielle T. ; Kayeyi, Nkomba ; Zulu, Paul M. ; Muzala, Kapina ; Mazaba, Mazyanga L. ; Hamoonga, Raymond ; Musonda, Kunda ; Monze, Mwaka ; Kapata, Nathan ; Sinyange, Nyambe ; Simwaba, Davie ; Kapaya, Fred ; Mulenga, Lloyd ; Chanda, Duncan ; Malambo, Warren ; Ngosa, William ; Hines, Jonas ; Yingst, Samuel ; Agolory, Simon ; Mukonka, Victor
-
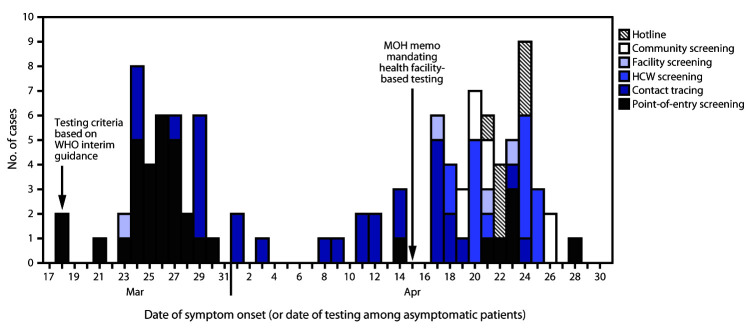
Description:Zambia is a landlocked, lower-middle income country in southern Africa, with a population of 17 million (1). The first known cases of coronaVirus disease 2019 (COVID-19) in Zambia occurred in a married couple who had traveled to France and were subject to port-of-entry Surveillance and subsequent remote monitoring of travelers with a History of international travel for 14 days after arrival. They were identified as having suspected cases on March 18, 2020, and tested for COVID-19 after developing respiratory symptoms during the 14-day monitoring period. In March 2020, the Zambia National Public Health Institute (ZNPHI) defined a suspected case of COVID-19 as 1) an acute respiratory illness in a person with a History of international travel during the 14 days preceding symptom onset; or 2) acute respiratory illness in a person with a History of contact with a person with laboratory-confirmed COVID-19 in the 14 days preceding symptom onset; or 3) severe acute respiratory illness requiring hospitalization; or 4) being a household or close contact of a patient with laboratory-confirmed COVID-19. This definition was adapted from World Health Organization (WHO) interim guidance issued March 20, 2020, on global Surveillance for COVID-19 (2) to also include asymptomatic contacts of persons with confirmed COVID-19. Persons with suspected COVID-19 were identified through various mechanisms, including port-of-entry Surveillance, contact tracing, health care worker (HCW) tTesting, facility-based inpatient screening, community-based screening, and calls from the public into a national hotline administered by the Disaster Management and Mitigation Unit and ZNPHI. Port-of-entry Surveillance included an arrival screen consisting of a temperature scan, report of symptoms during the preceding 14 days, and collection of a History of travel and contact with persons with confirmed COVID-19 in the 14 days before arrival in Zambia, followed by daily remote telephone monitoring for 14 days. Travelers were tested for SARS-CoV-2, the Virus that causes COVID-19, if they were symptomatic upon arrival or developed symptoms during the 14-day monitoring period. Persons with suspected COVID-19 were tested as soon as possible after evaluation for respiratory symptoms or within 7 days of last known exposure (i.e., travel or contact with a confirmed case). All COVID-19 diagnoses were confirmed using real-time reverse transcription-polymerase chain reaction (RT-PCR) tTesting (SARS-CoV-2 Nucleic Acid Detection Kit, Maccura) of nasopharyngeal specimens; all patients with confirmed COVID-19 were admitted into institutional isolation at the time of laboratory confirmation, which was generally within 36 hours. COVID-19 patients were deemed recovered and released from isolation after two consecutive PCR-negative test results ≥24 hours apart. A Ministry of Health memorandum was released on April 13, 2020, mandating tTesting in public facilities of 1) all persons admitted to medical and pediatric wards regardless of symptoms; 2) all patients being admitted to surgical and obstetric wards, regardless of symptoms; 3) any outpatient with fever, cough, or shortness of breath; and 4) any facility or community death in a person with respiratory symptoms, and 5) biweekly screening of all HCWs in isolation centers and health facilities where persons with COVID-19 had been evaluated. This report describes the first 100 COVID-19 cases reported in Zambia, during March 18-April 28, 2020.
-
Subjects:
-
Source:MMWR Morbidity Mortal Weekly Rep. 69(42):1547-1548
-
Series:
-
ISSN:0149-2195 (print) ; 1545-861X (digital)
-
Pubmed ID:33090982
-
Pubmed Central ID:PMC7583505
-
Document Type:
-
Place as Subject:
-
Pages in Document:2 pdf pages
-
Volume:69
-
Issue:42
-
Collection(s):
-
Main Document Checksum:urn:sha-512:4f6692fdd357639237977505487890b4be168303cc7931f4bfa603d9f511a7c54c0434037e1d2e7a6fba185d9be918d2c933414db68a8338654099aa97c7508c
-
Download URL:
-
File Type:
 [PDF
- 94.72 KB
]
[PDF
- 94.72 KB
]
Supporting Files

File Language:
English

{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
Morbidity and Mortality Weekly Report (MMWR)