215. Invasive Group A Streptococcus-Associated Hospitalizations and Risk Factors for In-Hospital Mortality Among Adults in California, 2000–2016
Supporting Files
Public Domain

-
October 23 2019
-
Details
-
Alternative Title:Open Forum Infect Dis
-
Personal Author:
-
Description:Background
Invasive group A Streptococcus (iGAS) causes severe illness and death but is not vaccine preventable or nationally notifiable. We describe the epidemiology of adult patients hospitalized with iGAS in California and risk factors for in-hospital death.
Methods
Using 2000–2016 California hospital discharge data, we extracted records for adults (≥18 years) with ≥1 group A Streptococcus (GAS)-associated International Classification of Diseases, Ninth or Tenth Revision discharge diagnosis code (e.g., unspecified GAS; GAS-specific pharyngitis, pneumonia, and sepsis) or known GAS-associated syndromes (e.g., acute rheumatic fever, erysipelas, scarlet fever). To identify patients hospitalized with iGAS, we selected extracted records that also had codes consistent with invasive disease (e.g., sepsis, pneumonia, intubation, or central line placement). We calculated iGAS-associated hospitalization incidence rates per 100,000 population and described patient demographics and comorbidities. We calculated the odds of in-hospital death using multivariable logistic regression (P < 0.05).
Results
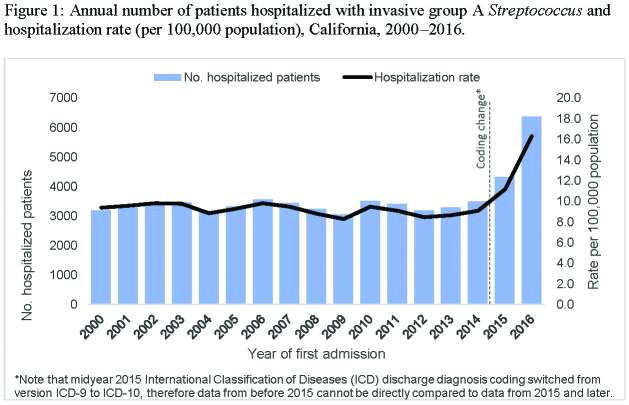
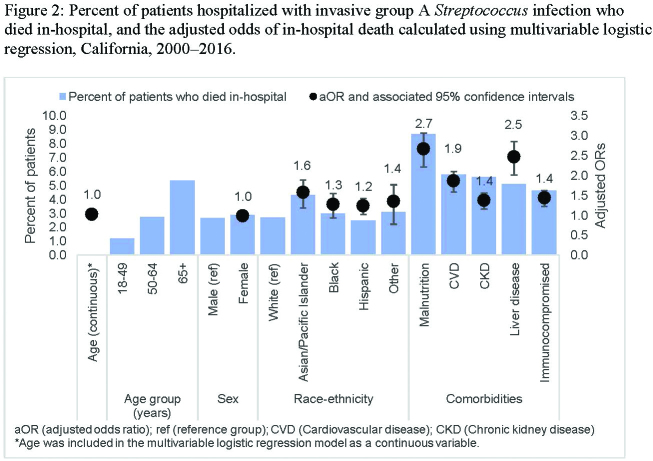
During 2000–2016 in California, 37,532 adults were hospitalized with iGAS; 1,045 (3%) died in-hospital. Mean annual hospitalization incidence was 9.4/100,000 population, and was highest (16.3/100,000) in 2016 (Figure 1). Most patients were male (56%), aged 40–65 (45%) or ≥65 (28%) years, and white (60%); 18% were immunocompromised. The percent of patients who died in-hospital increased with age and was highest among those with comorbidities such as malnutrition, cardiovascular disease (CVD), and chronic kidney disease (CKD) (Figure 2). In a multivariable model including age as a continuous variable, sex, and race-ethnicity, the odds of in-hospital death was significantly increased for patients with diagnosis codes for malnutrition, liver disease, CVD, immunosuppression, and CKD (Figure 2); within the race/ethnicity variable Asian/Pacific Islander patients had a higher odds of death compared with white patients.
Conclusion
Hospitalization and subsequent in-hospital death due to iGAS is substantial in California. Adults with iGAS who have specific comorbidities are at greater risk for death when hospitalized with iGAS.
Disclosures
All authors: No reported disclosures.
-
Subjects:
-
Source:Open Forum Infect Dis. 2019; 6(Suppl 2):S126-S127
-
Pubmed Central ID:PMC6809597
-
Document Type:
-
Volume:6
-
Collection(s):
-
Main Document Checksum:urn:sha256:9adf52de2236ea0e044491461bb67682f7129b642d658a6d2849f01332e6347f
-
Download URL:
-
File Type:
 [PDF
- 1.61 MB
]
[PDF
- 1.61 MB
]
Supporting Files

ON THIS PAGE

{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access