894. Universal Decolonization in Nursing Homes: Effect of Chlorhexidine and Nasal Povidone–Iodine on Prevalence of Multi-Drug-Resistant Organisms (MDROs) in the PROTECT Trial
Supporting Files
Public Domain

-
October 23 2019
-
Details
-
Alternative Title:Open Forum Infect Dis
-
Personal Author:Miller, Loren G ; McKinnell, James A ; Singh, Raveena ; Gussin, Gabrielle ; Kleinman, Ken ; Saavedra, Raheeb ; Mendez, Job ; Catuna, Tabitha D ; Felix, James ; Heim, Lauren ; Franco, Ryan ; Estevez, Marlene ; Lewis, Brian ; Shimabukuro, Julie ; Evans, Kaye ; Bittencourt, Cassiana ; Lee, Eunjung ; He, Jiayi ; Tjoa, Thomas ; Baesu, Christine ; Robinson, Philip A ; Tam, Steven ; Park, Steven ; Steinberg, Karl ; Beecham, Nancy ; Montgomery, Jocelyn ; Walters, DeAnn ; Stone, Nimalie D ; Huang, Susan S
-
Description:Background
The prevalence of MDROs in nursing homes (NH) is much higher than that of hospitals. Decolonization to reduce the reservoir of MDRO carriage in NH residents may be a strategy to address MDRO spread within and among healthcare facilities.
Methods
PROTECT is an 18-month cluster randomized trial of 1:1 universal decolonization vs. routine care in 28 NHs in California. Decolonization consists of chlorhexidine (CHG) bathing plus twice daily nasal iodophor on admission and Monday–Friday biweekly. We assessed pre- vs. post-intervention MDRO prevalence by sampling 50 randomly selected residents at each NH as an outcome unrelated to the trial’s primary intent (infection, hospitalization reduction). NH residents had nasal swabs cultured for methicillin-resistant S. aureus (MRSA), and skin (axilla/groin) swabs taken for MRSA, vancomycin-resistant Enterococcus (VRE), extended-spectrum β-lactamase producers (ESBL), and carbapenem-resistant Enterobacteriaceae (CRE). Generalized linear mixed models (GLM) assessed the difference in differences of MDRO prevalence using an arm by period interaction term, clustering by NH.
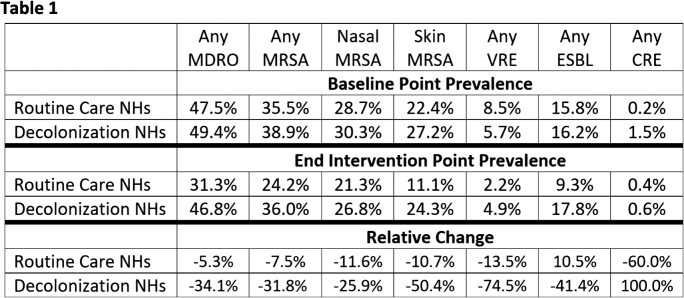
Results
Four NHs dropped from the trial. Among the 24 NHs that remained, MDRO colonization at baseline was 49.4% and 47.5% of residents in control (N = 650) vs. decolonization (N = 550) NHs, with no difference in MRSA, VRE, ESBL, and CRE (Table 1). Among remaining NHs, decolonization was associated with 28.8% raw decrease in MDRO prevalence in decolonization sites (GLM OR = 0.51, P < 0.001), 24.3% raw decrease in MRSA (OR = 0.66, P = 0.03), 61.0% raw decrease in VRE (OR = 0.17, P < 0.001), and 51.9% raw decrease in ESBL (OR = 0.40, P < 0.001). CRE increased, but numbers were small (Control arm: 10 in baseline, 4 in intervention; intervention arm: 1 in baseline, 2 in intervention, P = NS).
Conclusion
Universal NH decolonization with CHG bathing and nasal iodophor resulted in a marked decrease in Gram-positive and Gram-negative MDRO prevalence. This decrease may lower MDRO acquisition, infection, and antibiotic use within NHs, as well as regional MDRO spread to other healthcare facilities.
Disclosures
All Authors: No reported Disclosures.
-
Subjects:
-
Source:Open Forum Infect Dis. 2019; 6(Suppl 2):S24
-
Pubmed Central ID:PMC6809310
-
Document Type:
-
Volume:6
-
Collection(s):
-
Main Document Checksum:urn:sha256:ddb67c7c3f290cdea41d9303c88ffeadc6f75cea512cde1e626101df203a1726
-
Download URL:
-
File Type:
 [PDF
- 576.19 KB
]
[PDF
- 576.19 KB
]
Supporting Files

ON THIS PAGE

{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access