94. Pneumonia Severity Scores Poorly Predict Severe Outcomes Among Adults Hospitalized with Influenza
Supporting Files
Public Domain

-
October 23 2019
-
Details
-
Alternative Title:Open Forum Infect Dis
-
Personal Author:Doyle, Joshua ; Garg, Shikha ; O’Halloran, Alissa ; Beacham, Lauren ; Cummings, Charisse N ; Herlihy, Rachel ; Yousey-Hindes, Kim ; Anderson, Evan J ; Monroe, Maya ; Kim, Sue ; Lynfield, Ruth ; Irizarry, Lourdes ; Spina, Nancy ; Bennett, Nancy M ; Hill, Mary ; Reed, Carrie ; Schaffner, William ; Talbot, Keipp ; Self, Wesley ; Williams, Derek
-
Description:Background
Influenza can lead to severe outcomes among adults hospitalized with influenza, and causes substantial annual morbidity and mortality. We evaluated the performance of validated pneumonia severity indices in predicting severe influenza-associated outcomes.
Methods
We conducted a multicenter study within CDC’s Influenza Hospitalization Surveillance Network (FluSurv-NET) which included adults (≥ 18 years) hospitalized with laboratory-confirmed influenza during the 2017–18 influenza season. Medical charts were abstracted to obtain data on vital signs and laboratory values at admission on a stratified random sample of cases at a subset of hospitals at 11 network sites. Estimates were weighted to reflect the probability of selection. Cases were assigned to low- and high-risk groups based on the CURB-65 (‘Confusion, Urea, Respiratory rate, Blood pressure, Age ≥65’) index (high-risk cutoff = score ≥ 3), and the Pneumonia Severity Index (PSI) (high-risk cutoff = category V). We calculated area under receiver operating characteristic curves (AUROC), sensitivity, and specificity to estimate the performance of each index in predicting severe outcome categories: (1) intensive care unit (ICU) admission, 2) noninvasive mechanical ventilation (NIMV), (3) mechanical ventilation (MV), vasopressors, extracorporeal membrane oxygenation (ECMO) and (4) death.
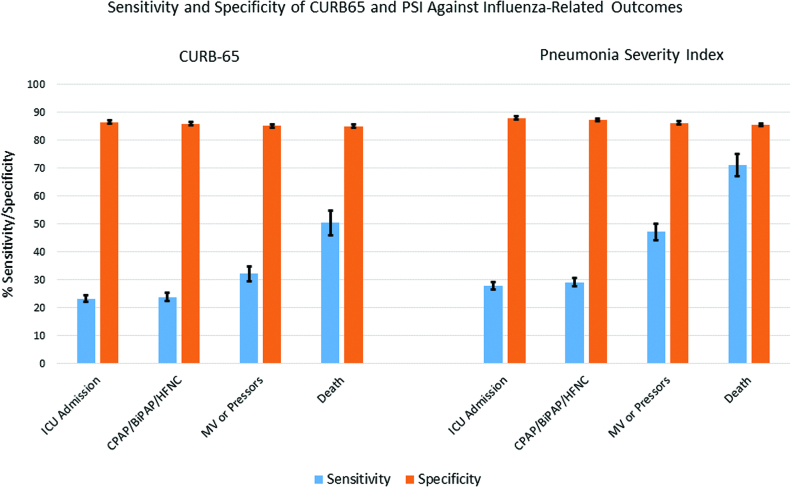
Results
Among 27,523 adults hospitalized with influenza, 8665 (31%) were sampled for inclusion in this analysis; median age was 70 years and 92% had ≥ 1 chronic condition. A total of 1,366 (16%) were classified as high-risk by CURB-65 and 1,249 (14%) by PSI. Both indices had low discrimination for severe outcomes; the AUROC for CURB-65 ranged from 0.55 for ICU admission to 0.65 for death, and for PSI ranged from 0.58 for ICU admission to 0.73 for death. Risk status by CURB-65 was less sensitive than PSI in predicting MV, vasopressor, or ECMO usage as well as death (figure). The specificity of CURB-65 and PSI was similar against all outcomes (figure).
Conclusion
The CURB-65 and PSI indices performed poorly in predicting severe outcomes other than death; PSI had the best discrimination overall. Alternative approaches are needed to predict severe influenza-related outcomes and optimize clinical care.
Disclosures
All Authors: No reported Disclosures.
-
Subjects:
-
Source:Open Forum Infect Dis. 2019; 6(Suppl 2):S8
-
Pubmed Central ID:PMC6809266
-
Document Type:
-
Volume:6
-
Collection(s):
-
Main Document Checksum:urn:sha256:566af2cb3c18fdaf5949d380e479ceec5405887bba38c998ab296d4e2f2cafa9
-
Download URL:
-
File Type:
 [PDF
- 211.32 KB
]
[PDF
- 211.32 KB
]
Supporting Files

ON THIS PAGE

{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access