Cost-effectiveness of increased influenza vaccination uptake against readmissions of major adverse cardiac events in the US
Supporting Files
Public Domain

-
April 29 2019
-
File Language:
English
Details
-
Alternative Title:PLoS One
-
Personal Author:
-
Description:Background
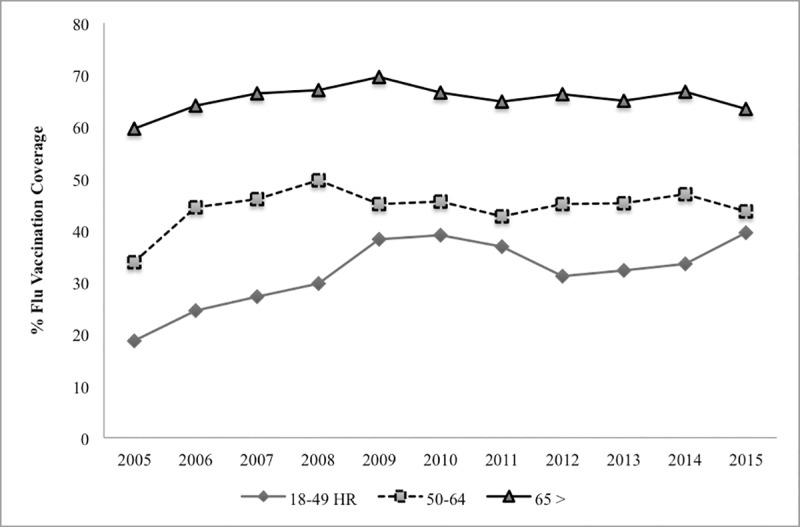
Although influenza vaccination has been shown to reduce the incidence of major adverse cardiac events (MACE) among those with existing cardiovascular disease (CVD), in the 2015–16 season, coverage for persons with heart disease was only 48% in the US.
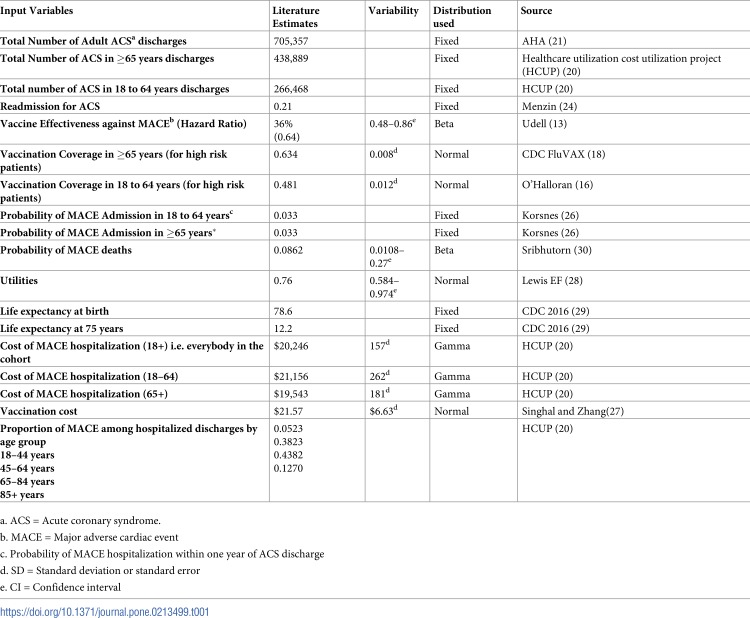
Methods
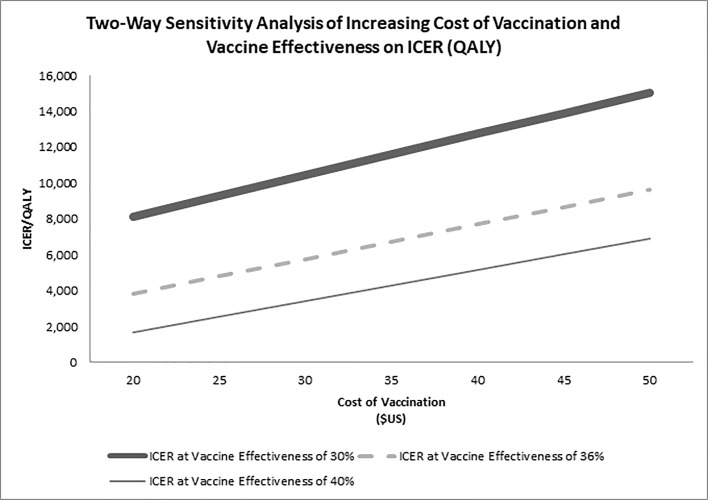
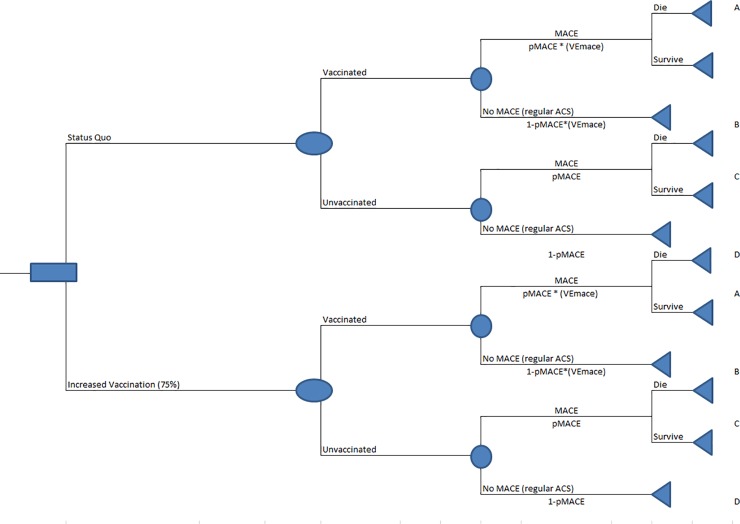
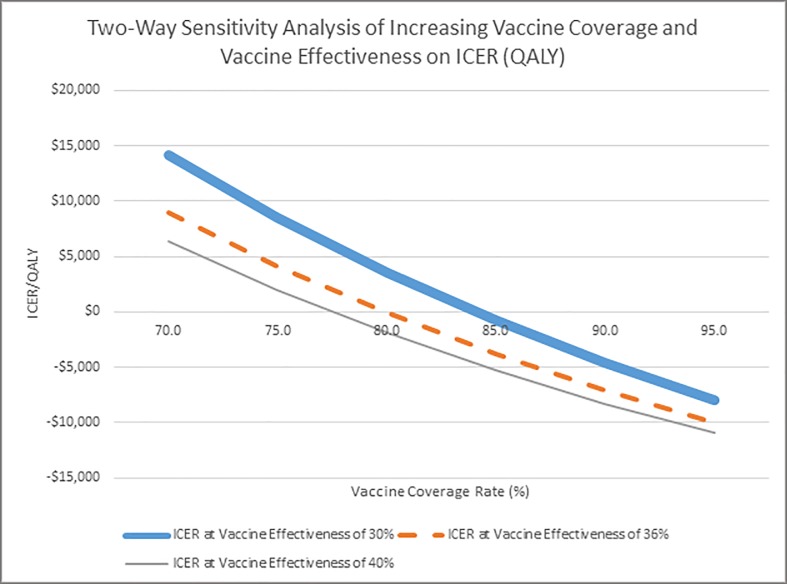
We built a Monte Carlo (probabilistic) spreadsheet-based decision tree in 2018 to estimate the cost-effectiveness of increased influenza vaccination to prevent MACE readmissions. We based our model on current US influenza vaccination coverage of the estimated 493,750 US acute coronary syndrome (ACS) patients from the healthcare payer perspective. We excluded outpatient costs and time lost from work and included only hospitalization and vaccination costs. We also estimated the incremental cost/MACE case averted and incremental cost/QALY gained (ICER) if 75% hospitalized ACS patients were vaccinated by discharge and estimated the impact of increasing vaccination coverage incrementally by 5% up to 95% in a sensitivity analysis, among hospitalized adults aged ≥ 65 years and 18–64 years, and varying vaccine effectiveness from 30–40%.
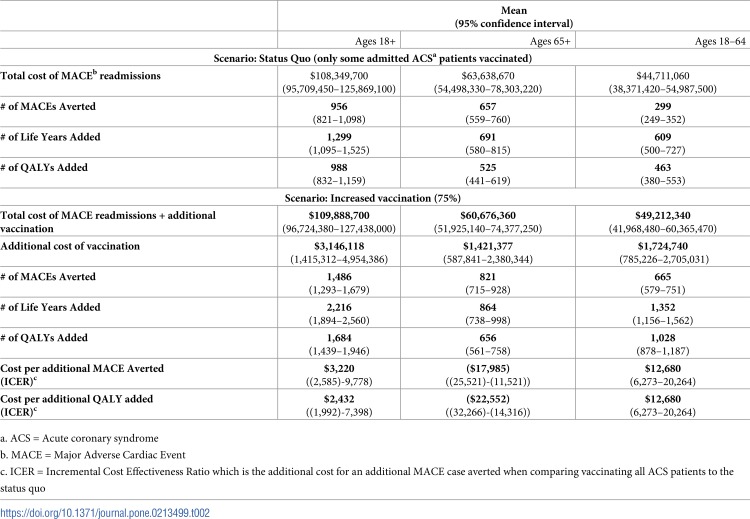
Result
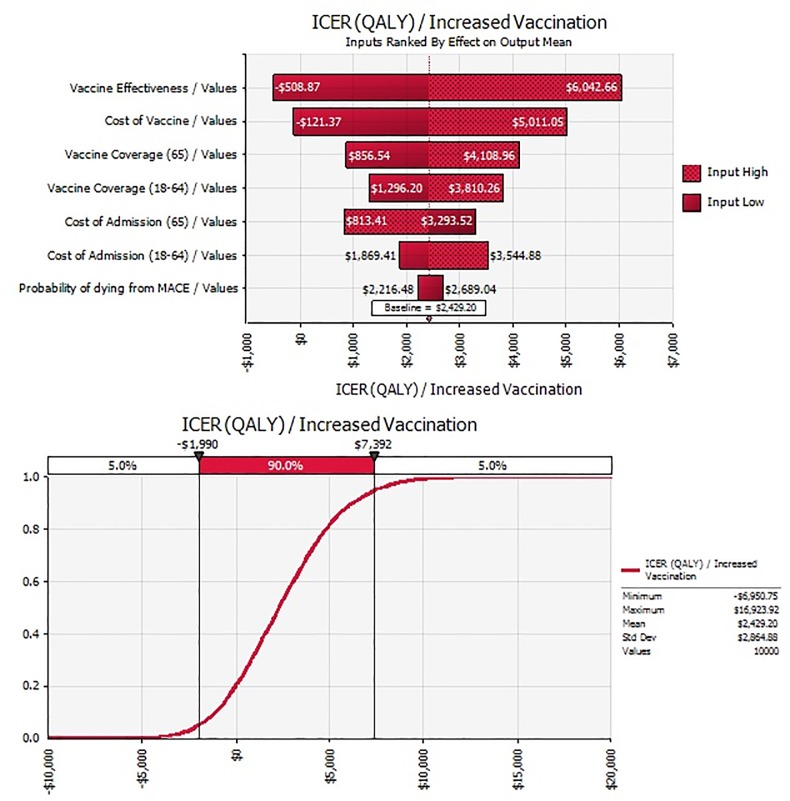
At 75% vaccination coverage by discharge, vaccination was cost-saving from the healthcare payer perspective in adults ≥ 65 years and the ICER was $12,680/QALY (95% CI: 6,273–20,264) in adults 18–64 years and $2,400 (95% CI: -1,992–7,398) in all adults 18 + years. These resulted in ~ 500 (95% CI: 439–625) additional averted MACEs/year for all adult patients aged ≥18 years and added ~700 (95% CI: 578–825) QALYs. In the sensitivity analysis, vaccination becomes cost-saving in adults 18+years after about 80% vaccination rate. To achieve 75% vaccination rate in all adults aged ≥ 18 years will require an additional cost of $3 million. The effectiveness of the vaccine, cost of vaccination, and vaccination coverage rate had the most impact on the results.
Conclusion
Increasing vaccination rate among hospitalized ACS patients has a favorable cost-effectiveness profile and becomes cost-saving when at least 80% are vaccinated.
-
Subjects:
-
Source:PLoS One. 14(4)
-
Pubmed ID:31034485
-
Pubmed Central ID:PMC6488048
-
Document Type:
-
Volume:14
-
Issue:4
-
Collection(s):
-
Main Document Checksum:urn:sha256:16f50bb76f3be89594b44d4e8635077398738759c85ebdfc6f19cf8115cb9d16
-
Download URL:
-
File Type:
 [PDF
- 1.37 MB
]
[PDF
- 1.37 MB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access