Key Collaborative Factors When Medicaid Accountable Care Organizations Work With Primary Care Clinics to Improve Colorectal Cancer Screening: Relationships, Data, and Quality Improvement Infrastructure
Supporting Files
Public Domain

-
August 15 2019
-
File Language:
English
Details
-
Journal Article:Preventing Chronic Disease (PCD)
-
Personal Author:
-
Description:Purpose
Accountable Care Organizations (ACOs) are implementing interventions to achieve triple-aim objectives of improved quality and experience of care while maintaining costs. Partnering across organizational boundaries is perceived as critical to ACO success.
Methods
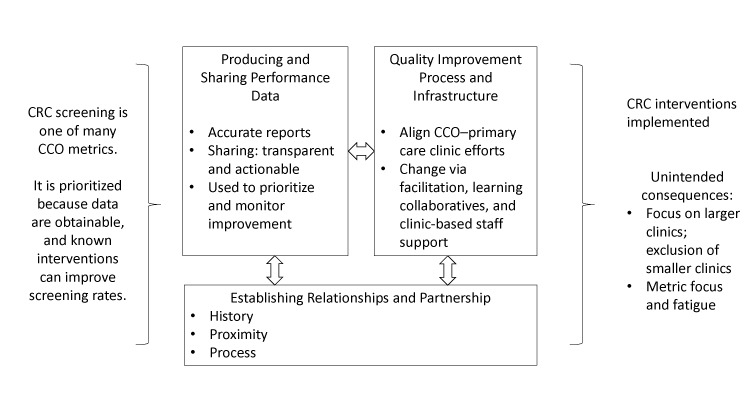
We conducted a comparative case study of 14 Medicaid ACOs in Oregon and their contracted primary care clinics using public performance data, key informant interviews, and consultation field notes. We focused on how ACOs work with clinics to improve colorectal cancer (CRC) screening — one incentivized performance metric.
Results
ACOs implemented a broad spectrum of multi-component interventions designed to increase CRC screening. The most common interventions focused on reducing structural barriers (n = 12 ACOs), delivering provider assessment and feedback (n = 11), and providing patient reminders (n = 7). ACOs developed their processes and infrastructure for working with clinics over time. Facilitators of successful collaboration included a history of and commitment to collaboration (partnership); the ability to provide accurate data to prioritize action and monitor improvement (performance data), and supporting clinics’ reflective learning through facilitation, learning collaboratives; and support of ACO as well as clinic-based staffing (quality improvement infrastructure). Two unintended consequences of ACO–clinic partnership emerged: potential exclusion of smaller clinics and metric focus and fatigue.
Conclusion
Our findings identified partnership, performance data, and quality improvement infrastructure as critical dimensions when Medicaid ACOs work with primary care to improve CRC screening. Findings may extend to other metric targets.
-
Subjects:
-
Source:Prev Chronic Dis. 16
-
ISSN:1545-1151
-
Pubmed ID:31418685
-
Pubmed Central ID:PMC6716418
-
Document Type:
-
Volume:16
-
Collection(s):
-
Main Document Checksum:urn:sha-512:8b11a58c7f8049bfa0e8eb41ffc33f37da792e29dc7cc27ff413d19b097ceff124752f8b8e3f1edcf3212464da914885ea574d0e13391951b320351ef554e27a
-
Download URL:
-
File Type:
 [PDF
- 360.62 KB
]
[PDF
- 360.62 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
Preventing Chronic Disease