Risk Factors for Invasive Methicillin-Resistant Staphylococcus aureus Infection After Recent Discharge From an Acute-Care Hospitalization, 2011–2013
Supporting Files

-
September 03 2015
-
File Language:
English
Details
-
Journal Article:Clin Infect Dis
-
Personal Author:Epstein, Lauren ; Mu, Yi ; Belflower, Ruth ; Scott, Janine ; Ray, Susan ; Dumyati, Ghinwa ; Felsen, Christina ; Petit, Susan ; Yousey-Hindes, Kimberly ; Nadle, Joelle ; Pasutti, Lauren ; Lynfield, Ruth ; Warnke, Linn ; Schaffner, William ; Leib, Karen ; Kallen, Alexander J. ; Fridkin, Scott K. ; Lessa, Fernanda C.
-
Description:Background.
Significant progress has been made in reducing methicillin-resistant Staphylococcus aureus (MRSA) infections among hospitalized patients. However, the decreases in invasive MRSA infections among recently discharged patients have been less substantial. To inform prevention strategies, we assessed risk factors for invasive MRSA infection after acute-care hospitalizations.
Methods.
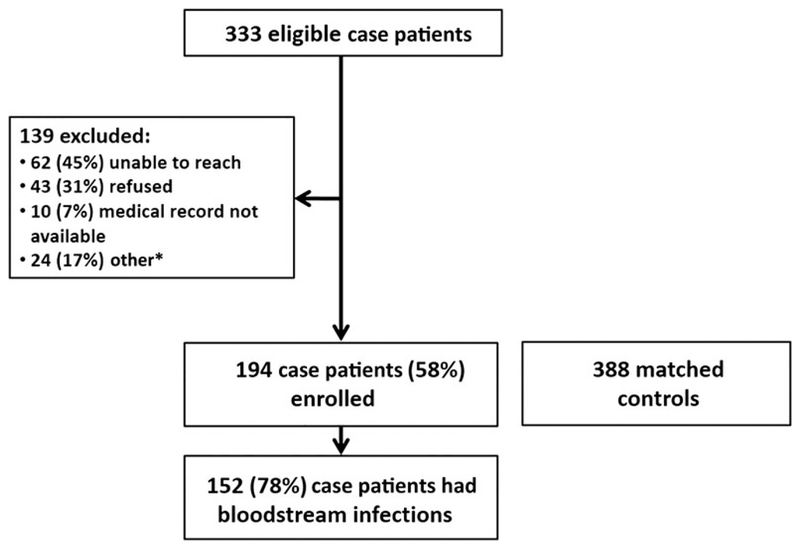
We conducted a prospective, matched case-control study. A case was defined as MRSA cultured from a normally sterile body site in a patient discharged from a hospital within the prior 12 weeks. Eligible case patients were identified from 15 hospitals across 6 US states. For each case patient, 2 controls were matched for hospital, month of discharge, and age group. Medical record reviews and telephone interviews were performed. Conditional logistic regression was used to identify independent risk factors for post-discharge invasive MRSA.
Results.
From 1 February 2011 through 31 March 2013, 194 case patients and 388 matched controls were enrolled. The median time between hospital discharge and positive culture was 23 days (range, 1–83 days). Factors independently associated with post-discharge MRSA infection included MRSA colonization (matched odds ratio [mOR], 7.71; 95% confidence interval [CI], 3.60–16.51), discharge to a nursing home (mOR, 2.65; 95% CI, 1.41–4.99), presence of a chronic wound during the post-discharge period (mOR, 4.41; 95% CI, 2.14–9.09), and discharge with a central venous catheter (mOR, 2.16; 95% CI, 1.13–4.99) or a different invasive device (mOR, 3.03; 95% CI, 1.24–7.39) in place.
Conclusions.
Prevention efforts should target patients with MRSA colonization or those with invasive devices or chronic wounds at hospital discharge. In addition, MRSA prevention efforts in nursing homes are warranted.
-
Subjects:
-
Source:Clin Infect Dis. 62(1):45-52
-
DOI:
-
Pubmed ID:26338787
-
Pubmed Central ID:PMC6557163
-
Document Type:
-
Funding:
-
Genre:
-
Volume:62
-
Issue:1
-
Collection(s):
-
Main Document Checksum:urn:sha-512:29a05071df5f7517a273769fd3d253d8ab4ed93425fff91a967047458d963322b4100155319bdaa7b1e3aa4ea045321dd6809eed065ab6b88c24a7405a0ee800
-
Download URL:
-
File Type:
 [PDF
- 231.27 KB
]
[PDF
- 231.27 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access