Morbidity and Mortality Weekly Report (MMWR): Surveillance Summaries, April 2019 / Vol. 68 / No. SS-3
Supporting Files
Public Domain

-
April 19, 2019
File Language:
English
Details
-
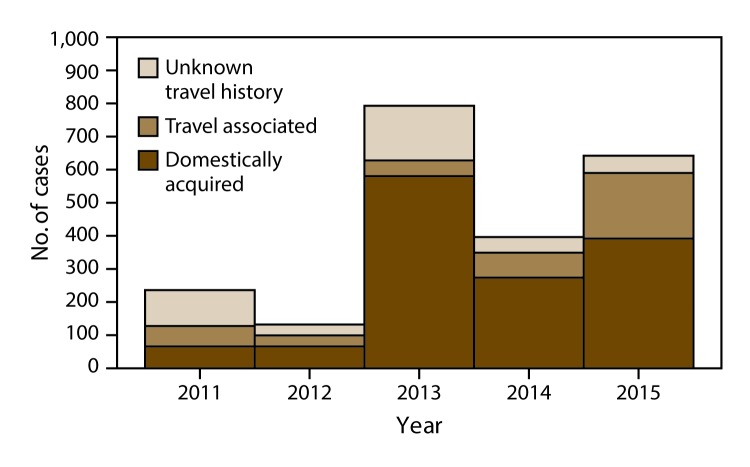
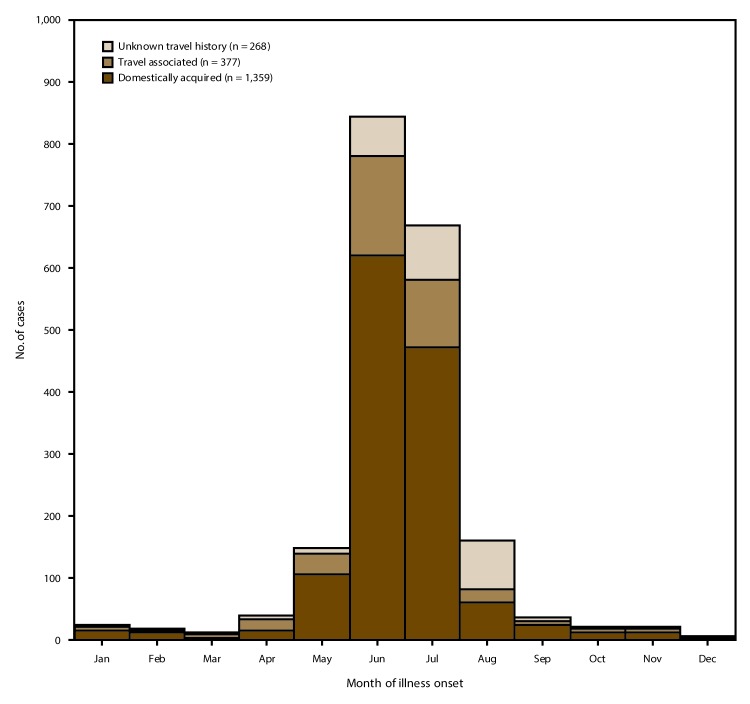
Alternative Title:Cyclosporiasis Surveillance — U.S. 2011–2015
-
Journal Article:Morbidity and Mortality Weekly Report (MMWR): Surveillance Summaries
-
Personal Author:
-
Corporate Authors:
-
Description:Cyclosporiasis is an intestinal illness caused by the parasite Cyclospora cayetanensis, which is transmissible by ingestion of fecally contaminated food or water. Cyclosporiasis is most common in tropical and subtropical regions of the world. In the U.S. foodborne outbreaks of cyclosporiasis have been linked to various types of imported fresh produce (e.g., basil, raspberries, and snow peas). Validated molecular typing tools, which could facilitate detection and investigation of outbreaks, are not yet available for C. cayetanensis.
CDC has been conducting national surveillance for cyclosporiasis since it became a nationally notifiable disease in January 1999. As of 2015, cyclosporiasis was a reportable condition in 42 states, the District of Columbia, and New York City (NYC). Health departments voluntarily notify CDC of cases of cyclosporiasis through the National Notifiable Diseases Surveillance System and submit additional case information using the CDC cyclosporiasis case report form or the Cyclosporiasis National Hypothesis Generating Questionnaire (CNHGQ).
-
Subjects:
-
Source:Morbidity and Mortality Weekly Report (MMWR): Surveillance Summaries, 2019; v. 68, no. 3
-
Series:
-
DOI:
-
ISSN:1546-0738 (print) ; 1545-8636 (digital)
-
Pubmed ID:31002104
-
Pubmed Central ID:PMC6476303
-
Document Type:
-
Place as Subject:
-
Pages in Document:16 pdf pages
-
Volume:68
-
Issue:3
-
Collection(s):
-
Main Document Checksum:urn:sha-512:5855800a0231231918e8bead347d295f25b1693496ad64e8ddf9e9b93f94410f928cf26b56052f5efaaabe41e6ef215aaa247cc62969988c2b373e4bca231b1f
-
Download URL:
-
File Type:
 [PDF
- 715.66 KB
]
[PDF
- 715.66 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
Morbidity and Mortality Weekly Report (MMWR)