Compliance with the National SEP-1 Quality Measure and Association with Sepsis Outcomes: A Multicenter Retrospective Cohort Study
Supporting Files

-
10 2018
-
File Language:
English
Details
-
Personal Author:Rhee, Chanu ; Filbin, Michael ; Massaro, Anthony F. ; Bulger, Amy ; McEachern, Donna ; Tobin, Kathleen A. ; Kitch, Barrett ; Thurlo-Walsh, Bert ; Kadar, Aran ; Koffman, Alexandra ; Pande, Anupam ; Hamad, Yasir ; Warren, David K. ; Jones, Travis ; O’Brien, Cara ; Anderson, Deverick J. ; Wang, Rui ; Klompas, Michael
-
Corporate Authors:
-
Description:Objectives
Many septic patients receive care that fails the Centers for Medicare and Medicaid Services’ SEP-1 measure, but it is unclear whether this reflects meaningful lapses in care, differences in clinical characteristics, or excessive rigidity of the “all-or-nothing” measure. We compared outcomes in cases that passed versus failed SEP-1 during the first 2 years after the measure was implemented.
Design
Retrospective cohort study.
Setting
Seven U.S. hospitals.
Patients
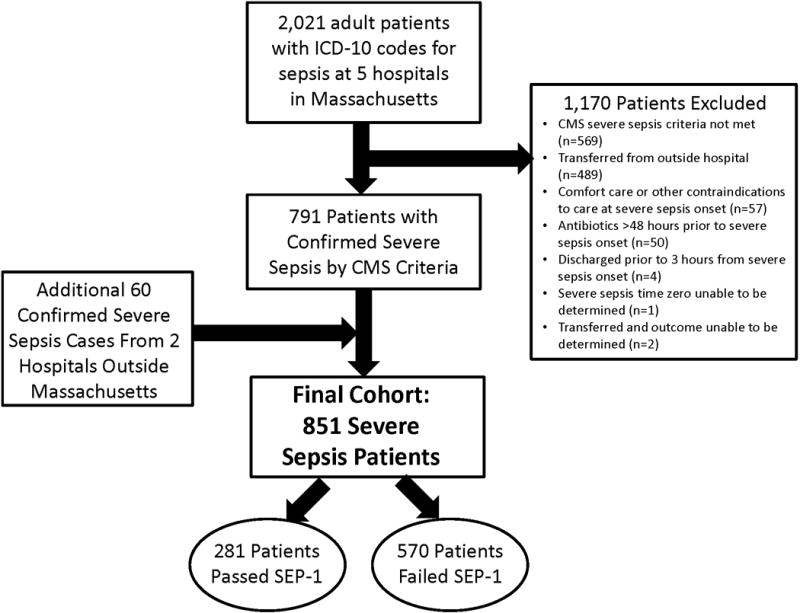
Adult patients included in SEP-1 reporting between October 2015 and September 2017.
Interventions
None.
Measurements and Main Results
Of 851 sepsis cases in the cohort, 281 (33%) passed SEP-1 and 570 (67%) failed. SEP-1 failures had higher rates of septic shock (20% vs 9%, p<0.001), hospital-onset sepsis (11% vs 4%, p=0.001), and vague presenting symptoms (46% vs 30%, p<0.001). The most common reasons for failure were omission of 3-hour and 6-hour lactate measurements (228/570 failures, 40%). Only 86/570 failures (15.1%) had >3-hour delays until broad-spectrum antibiotics. Cases that failed SEP-1 had higher in-hospital mortality rates (18.4% vs 11.0%, OR 1.82, 95% CI 1.19-2.80, p=0.006) but this association was no longer significant after adjusting for differences in clinical characteristics and severity-of-illness (adjusted OR 1.36, 95% CI 0.85-2.18, p=0.205). Delays of >3-hours until antibiotics were significantly associated with death (adjusted OR 1.94, 95% CI 1.04-3.62, p=0.038) while failing SEP-1 for any other reason was not (adjusted OR 1.10, 95% CI 0.70-1.72, p=0.674).
Conclusions
Crude mortality rates were higher in sepsis cases that failed versus passed SEP-1 but there was no difference after adjusting for clinical characteristics and severity-of-illness. Delays in antibiotic administration were associated with higher mortality but only accounted for a small fraction of SEP-1 failures. SEP-1 may not clearly differentiate between high versus low-quality care and detailed risk adjustment is necessary to properly interpret associations between SEP-1 compliance and mortality.
-
Keywords:
-
Source:Crit Care Med. 46(10):1585-1591
-
Pubmed ID:30015667
-
Pubmed Central ID:PMC6138564
-
Document Type:
-
Funding:
-
Volume:46
-
Issue:10
-
Collection(s):
-
Main Document Checksum:urn:sha-512:6cf2fdc085fbddc8d46c15819646fba938576d1743f02f13b01f2463de12de17e734ffe68790eaa51cc84e61ae09c45bb491e86501a28a48b7e3b4026f7a0e4a
-
Download URL:
-
File Type:
 [PDF
- 203.11 KB
]
[PDF
- 203.11 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access