Multiple Naloxone Administrations Among Emergency Medical Service Providers is Increasing
Supporting Files

-
2017
-
File Language:
English
Details
-
Alternative Title:Prehosp Emerg Care
-
Personal Author:
-
Description:Background
Opioid overdoses are at epidemic levels in the United States. Emergency Medical Service (EMS) providers may administer naloxone to restore patient breathing and prevent respiratory arrest. There was a need for contemporary data to examine the number of naloxone administrations in an EMS encounter.
Methods
Using data from the National Emergency Medical Services Information System, we examined data from 2012–5 to determine trends in patients receiving multiple naloxone administrations (MNAs). Logis tic regression including demographic, clinical, and operational information was used to examine factors associated with MNA.
Results
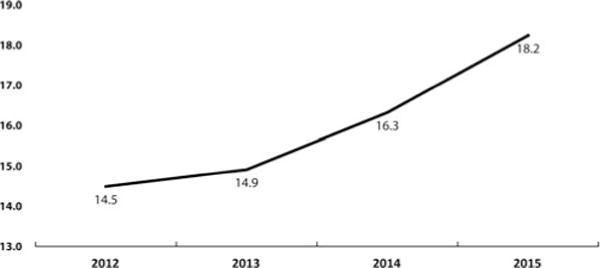
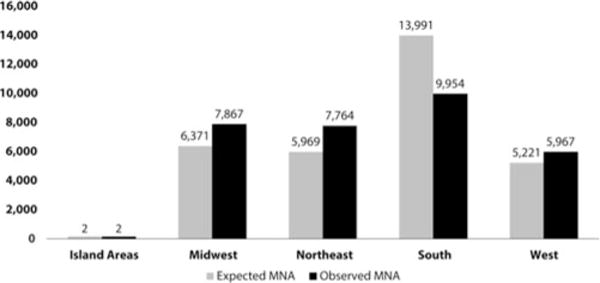
Among all events where naloxone was administered only 16.7% of the 911 calls specifically identified the medical emergency as a drug ingestion or poisoning event. The percentage of patients receiving MNA increased from 14.5% in 2012 to 18.2% in 2015, which represents a 26% increase in MNA in 4 years. Patients aged 20–29 had the highest percentage of MNA (21.1%). Patients in the Northeast and the Midwest had the highest relative MNA (Chi Squared = 539.5, p < 0.01 and Chi Squared = 351.2, p < 0.01, respectively). The logistic regression model showed that the adjusted odds ratios (aOR) for MNA were greatest among people who live in the Northeast (aOR = 1.18, 95% CI = 1.13–1.22) and for men (aOR = 1.13, 95% CI = 1.10–1.16), but lower for suburban and rural areas (aOR = 0.76, 95% CI = 0.72–0.80 and aOR = 0.85, 95% CI = 0.80–0.89) and lowest for wilderness areas (aOR = 0.76, 95% CI = 0.68–0.84). Higher adjusted odds of MNA occurred when an advanced life support (ALS 2) level of service was provided compared to basic life support (BLS) ambulances (aOR = 2.15, 95% CI = 1.45–3.16) and when the dispatch complaint indicated there was a drug poisoning event (aOR = 1.12, 95% CI = 1.09–1.16). Reported layperson naloxone administration prior to EMS arrival was rare (1%).
Conclusion
This study shows that frequency of MNA is growing over time and is regionally dependent. MNA may be a barometer of the potency of the opioid involved in the overdose. The increase in MNAprovides support for a dosage review. Better identification of opioid related events in the dispatch system could lead to a better match of services with patient needs.
-
Subjects:
-
Keywords:
-
Source:Prehosp Emerg Care. 21(4):411-419
-
Pubmed ID:28481656
-
Pubmed Central ID:PMC6026856
-
Document Type:
-
Funding:
-
Volume:21
-
Issue:4
-
Collection(s):
-
Main Document Checksum:urn:sha-512:26354b82ac38cf2276b88f62d5fcc5be89223ccfe234946ad53daa672f8b4b7e61d12060f8ef2f2474f8c44990603881cf63efc62dc6e1aa743b0e2a72a1e608
-
Download URL:
-
File Type:
 [PDF
- 377.92 KB
]
[PDF
- 377.92 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access