Agreement between self-reported and physically verified male circumcision status in Nyanza region, Kenya: Evidence from the TASCO study
Supporting Files

-
Feb 12 2018
-
File Language:
English
Details
-
Alternative Title:PLoS One
-
Personal Author:
-
Description:Background
Self-reported male circumcision (MC) status is widely used to estimate community prevalence of circumcision, although its accuracy varies in different settings depending on the extent of misreporting. Despite this challenge, self-reported MC status remains essential because it is the most feasible method of collecting MC status data in community surveys. Therefore, its accuracy is an important determinant of the reliability of MC prevalence estimates based on such surveys. We measured the concurrence between self-reported and physically verified MC status among men aged 25–39 years during a baseline household survey for a study to test strategies for enhancing MC uptake by older men in Nyanza region of Kenya. The objective was to determine the accuracy of self-reported MC status in communities where MC for HIV prevention is being rolled out.
Methods
Agreement between self-reported and physically verified MC status was measured among 4,232 men. A structured questionnaire was used to collect data on MC status followed by physical examination to verify the actual MC status whose outcome was recorded as fully circumcised (no foreskin), partially circumcised (foreskin is past corona sulcus but covers less than half of the glans) or uncircumcised (foreskin covers half or more of the glans). The sensitivity and specificity of self-reported MC status were calculated using physically verified MC status as the gold standard.
Results
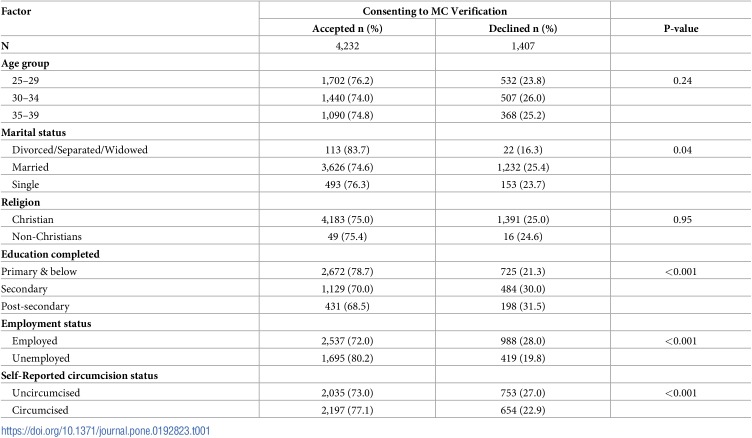
Out of 4,232 men, 2,197 (51.9%) reported being circumcised, of whom 99.0% were confirmed to be fully circumcised on physical examination. Among 2,035 men who reported being uncircumcised, 93.7% (1,907/2,035) were confirmed uncircumcised on physical examination. Agreement between self-reported and physically verified MC status was almost perfect, kappa (k) = 98.6% (95% CI, 98.1%-99.1%. The sensitivity of self-reporting being circumcised was 99.6% (95% CI, 99.2–99.8) while specificity of self-reporting uncircumcised was 99.0% (95% CI, 98.4–99.4) and did not differ significantly by age group based on chi-square test. Rate of consenting to physical verification of MC status differed by client characteristics; unemployed men were more likely to consent to physical verification (odds ratio [OR] = 1.48, (95% CI, 1.30–1.69) compared to employed men and those with post-secondary education were less likely to consent to physical verification than those with primary education or less (odds ratio [OR] = 0.61, (95% CI, 0.51–0.74).
Conclusions
In this Kenyan context, both sensitivity and specificity of self-reported MC status was high; therefore, MC prevalence estimates based on self-reported MC status should be deemed accurate and applicable for planning. However MC programs should assess accuracy of self-reported MC status periodically for any secular changes that may undermine its usefulness for estimating community MC prevalence in their unique settings.
-
Subjects:
-
Source:PLoS One. 13(2).
-
Pubmed ID:29432444
-
Pubmed Central ID:PMC5809057
-
Document Type:
-
Funding:
-
Place as Subject:
-
Volume:13
-
Issue:2
-
Collection(s):
-
Main Document Checksum:urn:sha256:6ea2060ae7cae517e5faa4c6fc536b1ee117099548c3f1a70a0a1be923aacfc7
-
Download URL:
-
File Type:
 [PDF
- 619.67 KB
]
[PDF
- 619.67 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access