Assessing The Impact of The National Healthcare Safety Network’s (NHSN’s) New Baseline on Acute Care Hospital Standardized Infection Ratios (SIRs)
Supporting Files
Public Domain

-
Oct 04 2017
-
Details
-
Alternative Title:Open Forum Infect Dis
-
Personal Author:
-
Description:Background
To more accurately measure the progress of healthcare-associated infection (HAI) prevention efforts, the CDC’s National Healthcare Safety Network (NHSN) surveillance system updated risk-adjustment models for computation of updated Standardized Infection Ratios (SIRs), the primary HAI summary measure by NHSN. This study sought to examine how the updated SIRs varied from the previous SIRs calculated using older baselines for acute care hospital HAIs.
Methods
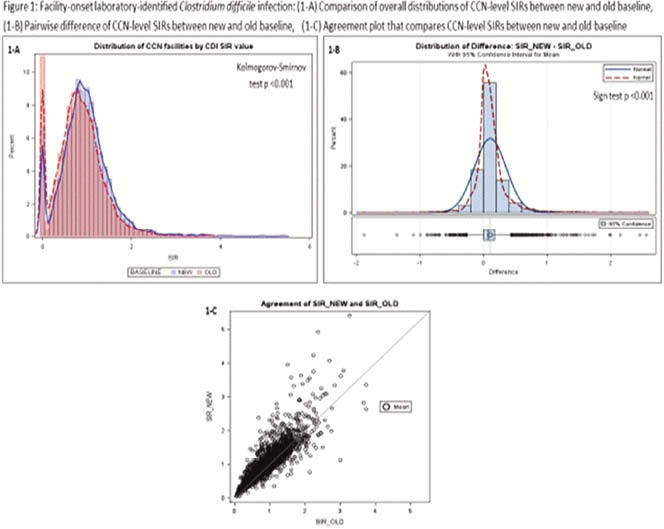
We analyzed NHSN data for healthcare facility-onset laboratory-identified Clostridium difficile [CDI] and methicillin-resistant Staphylococcus aureus [MRSA] bacteremia reported in accordance with the CMS’ inpatient quality reporting program requirement. The unit of analysis was CMS certification number (CCN) facility reporting in 2015. We compared overall distributions of CCN-level SIRs (CCN-SIRs) between new risk-adjustment models using a 2015 baseline (SIR_NEW) and old models using a 2011 baseline (SIR_OLD) and tested location shift (median away from null) of pairwise differences. We also examined the magnitude of shift in SIR from old to new baseline.
Results
For each HAI, the national pooled mean SIR of the new baseline was ~1.0. For CDI, the overall distributions of CCN SIR_NEW and CCN-SIR_OLD were different, and the median of pairwise difference was away from null with CCN-SIR_NEW slightly higher. For MRSA, the SIR differences were not significant. Most CCN-SIRs (83% for CDI, 93% for MRSA) remained in the same significance category across the old and new baselines (“worse,” “better, ‘not different from national benchmark’), and few CCN-SIRs were reclassified to a less favorable category. For 75% of CCN-SIRs, their relative position in the quartile distributions of SIR_NEW and SIR_OLD remained the same. The discrepancies between SIR_NEW and SIR_OLD tended to be larger among CCNs with high SIRs.
Conclusion
The updated national pooled mean SIRs were close to 1.0, validating the potential use of new risk adjustment models and baseline as updated benchmarks for tracking CDI and MRSA prevention progress. The shifts in CCN-level SIRs between old and new baselines were not large, indicating a modest impact of new baselines at the CCN level, except among hospitals with high SIRs.
Disclosures
All authors: No reported disclosures.
-
Subjects:
-
Source:Open Forum Infect Dis. 2017; 4(Suppl 1):S49-S50.
-
Pubmed Central ID:PMC5632249
-
Document Type:
-
Volume:4
-
Collection(s):
-
Main Document Checksum:urn:sha256:df7aa9fbe3cd08949274cd73f68214eb26fedfba92282c99017d32c2f21e821c
-
Download URL:
-
File Type:
 [PDF
- 693.08 KB
]
[PDF
- 693.08 KB
]
Supporting Files

ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access