Quantification of CD4 Responses to Combined Antiretroviral Therapy Over 5 Years Among HIV-Infected Children in Kinshasa, Democratic Republic of Congo
Supporting Files

-
9 01 2012
-
File Language:
English
Details
-
Alternative Title:J Acquir Immune Defic Syndr
-
Personal Author:
-
Description:Background
The long-term effects of combined antiretroviral therapy (cART) on CD4 percentage in HIV-infected children are incompletely understood, with evidence from resource-deprived areas particularly scarce even though most children with HIV live in such settings. We sought to describe this relationship.
Methods
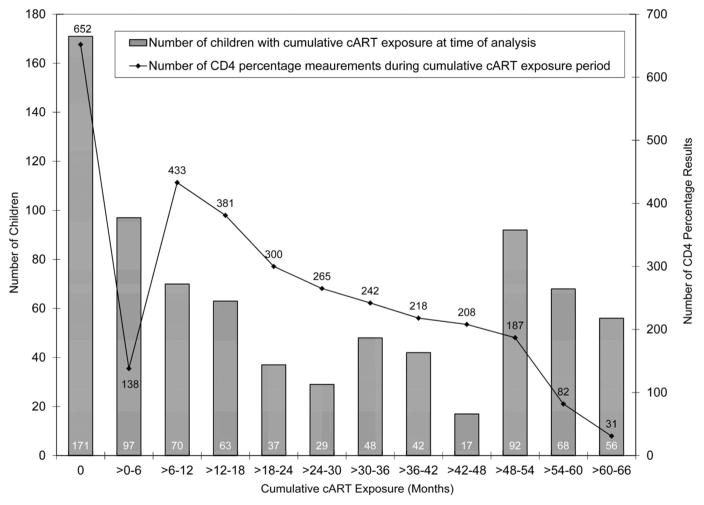
Observational longitudinal data from cART-naive children enrolled between December 2004 and May 2010 into an HIV care and treatment program in Kinshasa, Democratic Republic of Congo were analyzed. To estimate the effect of cART on CD4 percentage while accounting for time-dependent confounders affected by prior exposure to cART, a marginal structural linear mean model was used.
Results
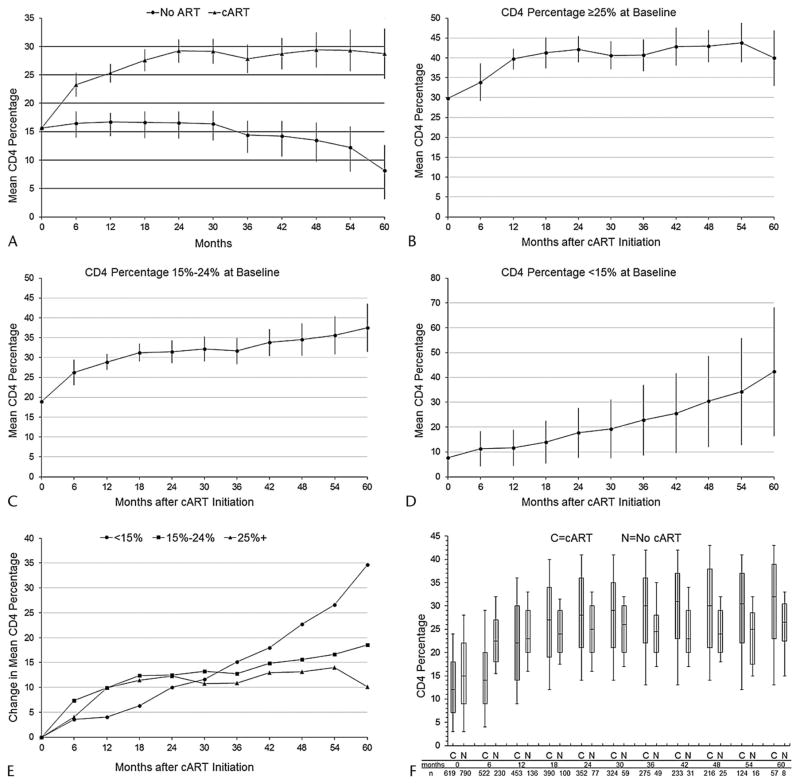
Seven hundred ninety children were active for 2090 person-years and a median of 31 months; 619 (78%) initiated cART. At baseline, 405 children (51%) were in HIV clinical stage 3 or 4; 528 (67%) had advanced or severe immunodeficiency. Compared with no cART, the estimated absolute rise in CD4 percentage was 6.8% [95% confidence interval (CI), 4.7% to 8.9%] after 6 months of cART, 8.6% (95% CI, 7.0% to 10.2%) after 12 months, and 20.5% (95% CI, 16.1% to 24.9%) after 60 months. cART-mediated CD4 percentage gains were slowest but greatest among children with baseline CD4 percentage <15. The cumulative incidence of recovery to “not significant” World Health Organization age-specific immunodeficiency was lower if cART was started when immunodeficiency was severe rather than mild or advanced.
Conclusions
cART increased CD4 percentages among HIV-infected children in a resource-deprived setting, as previously noted among children in the United States. More gradual and protracted recovery in children with lower baseline CD4 percentages supports earlier initiation of pediatric cART.
-
Keywords:
-
Source:J Acquir Immune Defic Syndr. 61(1):90-98
-
Pubmed ID:22732464
-
Pubmed Central ID:PMC5592966
-
Document Type:
-
Funding:
-
Volume:61
-
Issue:1
-
Collection(s):
-
Main Document Checksum:urn:sha256:b67e05a82503b240168a3eda1b8e8f9e045eb9452706ce1c92bf4c10497f6cfe
-
Download URL:
-
File Type:
 [PDF
- 565.25 KB
]
[PDF
- 565.25 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access