Measuring the impact of seasonal malaria chemoprevention as part of routine malaria control in Kita, Mali
Supporting Files
Public Domain

-
Aug 10 2017
-
Details
-
Alternative Title:Malar J
-
Personal Author:
-
Description:Background
Seasonal malaria chemoprevention (SMC) is a new strategy recommended by WHO in areas of highly seasonal transmission in March 2012. Although randomized controlled trials (RCTs) have shown SMC to be highly effective, evidence and experience from routine implementation of SMC are limited.
Methods
A non-randomized pragmatic trial with pre-post design was used, with one intervention district (Kita), where four rounds of SMC with sulfadoxine + amodiaquine (SP + AQ) took place in August–November 2014, and one comparison district (Bafoulabe). The primary aims were to evaluate SMC coverage and reductions in prevalence of malaria and anaemia when SMC is delivered through routine programmes using existing community health workers. Children aged 3–59 months from 15 selected localities per district, sampled with probability proportional to size, were surveyed and blood samples collected for malaria blood smears, haemoglobin (Hb) measurement, and molecular markers of drug resistance in two cross-sectional surveys, one before SMC (July 2014) and one after SMC (December 2014). Difference-in-differences regression models were used to assess and compare changes in malaria and anaemia in the intervention and comparison districts. Adherence and tolerability of SMC were assessed by cross-sectional surveys 4–7 days after each SMC round. Coverage of SMC was assessed in the post-SMC survey.
Results
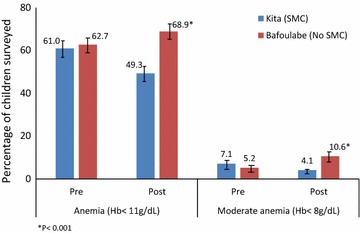
During round 1, 84% of targeted children received at least the first SMC dose, but coverage declined to 67% by round 4. Across the four treatment rounds, 54% of children received four complete SMC courses. Prevalence of parasitaemia was similar in intervention and comparison districts prior to SMC (23.4 vs 29.5%, p = 0.34) as was the prevalence of malaria illness (2.4 vs 1.9%, p = 0.75). After SMC, parasitaemia prevalence fell to 18% in the intervention district and increased to 46% in the comparison district [difference-in-differences (DD) OR = 0.35; 95% CI 0.20–0.60]. Prevalence of malaria illness fell to a greater degree in the intervention district versus the comparison district (DD OR = 0.20; 95% CI 0.04–0.94) and the same for moderate anaemia (Hb < 8 g/dL) (DD OR = 0.26, 95% CI 0.11–0.65). The frequency of the quintuple mutation (dhfr N51I, C59R and S108N + dhps A437G and K540E) remained low (5%) before and after intervention in both districts.
Conclusions
Routine implementation of SMC in Mali substantially reduced malaria and anaemia, with reductions of similar magnitude to those seen in previous RCTs. Improving coverage could further strengthen SMC impact.
-
Subjects:
-
Source:Malar J. 16.
-
Pubmed ID:28797263
-
Pubmed Central ID:PMC5553795
-
Document Type:
-
Volume:16
-
Collection(s):
-
Main Document Checksum:urn:sha256:173d980ecf754a57af4ef27ac9aefdd8cf3c3e4349435d4f94d84b75de4c7701
-
Download URL:
-
File Type:
 [PDF
- 1.21 MB
]
[PDF
- 1.21 MB
]
Supporting Files

ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access